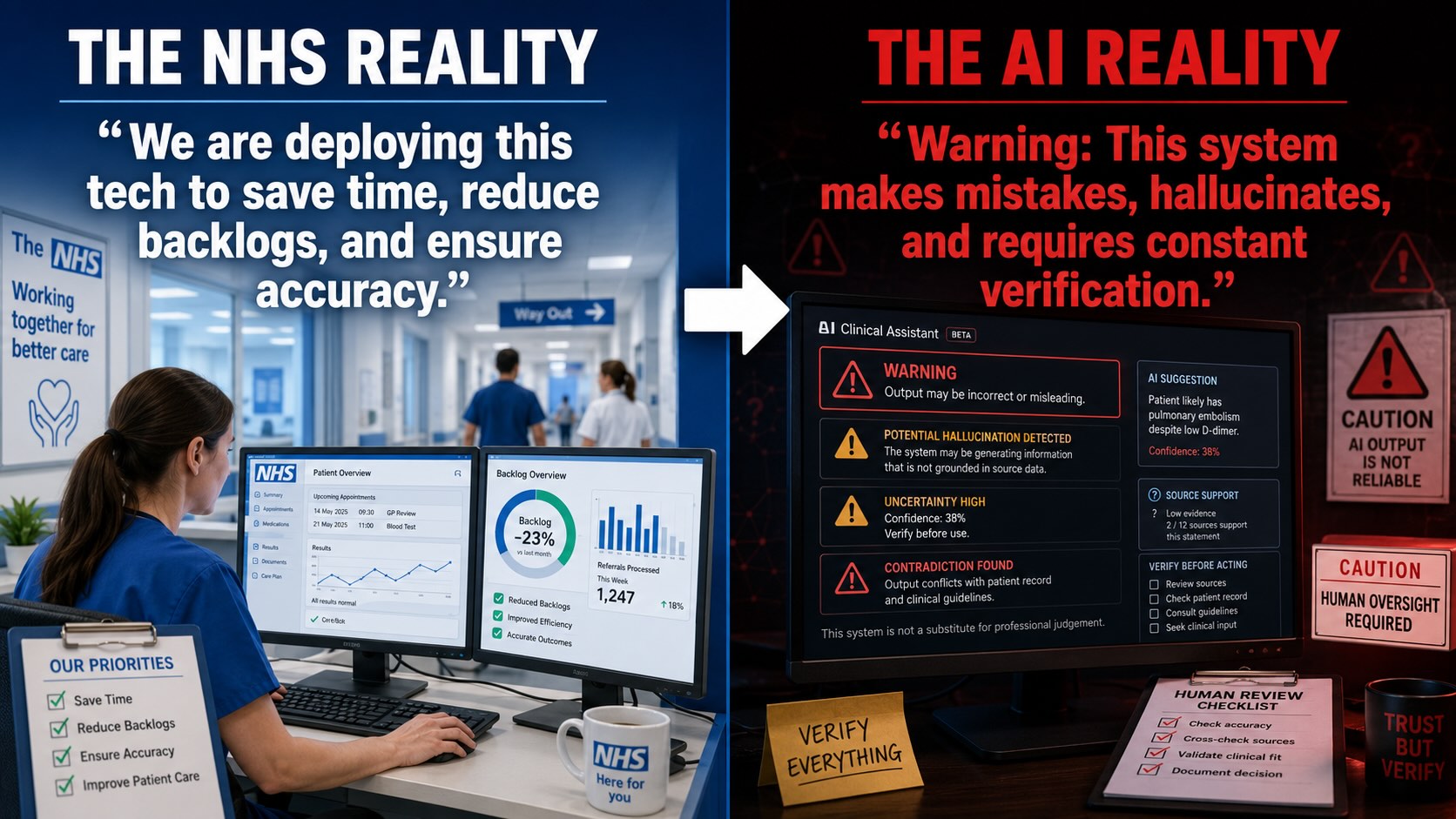
Figure A. NHS Operational Objectives Compared with the Inherent Limitations of Generative AI. This illustrative figure contrasts the NHS objective of improving efficiency, reducing backlogs and supporting accurate clinical workflows with the inherent characteristics of generative AI systems, which may produce inaccurate outputs, hallucinations, uncertainty and unsupported inferences that require continuous human verification. The comparison demonstrates that AI-generated outputs are probabilistic and should not be treated as authoritative clinical decisions without appropriate governance, independent validation, documented human oversight and clinical review. It introduces the central issue examined throughout this disclosure: the distinction between organisational expectations of AI and the operational safeguards necessary to ensure patient safety, accountability and lawful processing of medical information.
Public Criminal-Threat Governance, AI-Mediated Patient Access, Voice / Accent Validation Failure, Data Execution Non-Disclosure, SaaS Dependency, Workforce Liability Displacement, and Patient-Record Risk
Mass NHS AI deployment is being advanced across patient access, clinical documentation, staff workflow, and administrative systems before the public record has visibly disclosed the processing engine, execution location, model logic, voice / accent validation, human-review pathway, clinical safety case, sovereignty assurance, worker-liability boundary, or patient-consent architecture.
Download PDF Breach Slides 1 - 18
Table of Contents
- Executive Summary
- Scope of This Disclosure
- Public-Interest Position
- Core Structural Contradiction
- Central Thesis
- Disclosure Position
- Working Breach Set
- Opening Conclusion
- Breach I — Public Criminal-Threat Governance and Staff Liability Displacement
- Breach II — Mass Named-User AI Licence Exposure and Audit-Trail Liability
- Breach III — AI Triage Processing Sovereignty and Undisclosed Decision Engine
- Breach IV — Data Execution, Modelling Location, and Cross-Border Data-Bleed Non-Disclosure
- Breach V — AI Triage Output Traceability, Accuracy, and Human-Review Failure
- Breach VI — Voice / Speech AI Accent Validation Failure and Unsafe National Scaling from Sussex Pilot Evidence
- Breach VII — Ambient Voice Technology and AI-Mediated Clinical Record Formation
- Breach VIII — Patient Consent, Transparency, and Meaningful Choice Failure
- Breach IX — Pseudonymisation, Re-Identification, and Pattern-Correlation Failure
- Breach X — Staff Digital Competence, Training, and Professionalisation Mismatch
- Breach XI — Clinical Safety Case, DPIA, Equality Impact, and Assurance Visibility Failure
- Breach XII — Patient Access Inequality and Digital Exclusion
- Breach XIII — Cybersecurity Blind Spot: Authorised Use as Exposure Pathway
- Breach XIV — AI Hallucination, Verification Burden, and Workforce Stress Risk
- Summary
- Evidence Supported
- Mechanism Identified
- Legal Frameworks Engaged
- Legal Duty
- Breach Identified
- Hallucination and Output-Reliance Risk
- Verification Burden Risk
- Workforce Stress Risk
- Clinical Record Risk
- Staff Liability Risk
- Tribunal / Procedural Risk
- Disclosure Questions
- Evidence Relied Upon
- Final Breach Position
- Breach XV — Vendor, Sub-Processor, Cloud, Telemetry, and Support-Access Disclosure Failure
- Breach XVI — Accountability Gap Between NHS England, ICBs, GP Practices, Vendors, and Staff
- Summary
- Evidence Supported
- Mechanism Identified
- Legal Frameworks Engaged
- Legal Duty
- Breach Identified
- Patient Redress Risk
- Staff Liability Risk
- Vendor Accountability Risk
- Controller / Processor Risk
- Clinical Safety Accountability Risk
- Tribunal / Procedural Risk
- Disclosure Questions
- Evidence Relied Upon
- Final Breach Position
- Breach XVII — AI Output Reliance in Employment, Disciplinary, Tribunal, and Protected-Disclosure Contexts
- Summary
- Evidence Supported
- Mechanism Identified
- Legal Frameworks Engaged
- Legal Duty
- Breach Identified
- Protected-Disclosure Risk
- Employment Disciplinary Risk
- Tribunal Evidence Risk
- Patient-Record Evidence Risk
- Data Accuracy and Rectification Risk
- Tribunal / Procedural Disclosure Requirements
- Disclosure Questions
- Evidence Relied Upon
- Final Breach Position
- Breach XVIII — Public-Sector AI Dependency, Foreign-Controlled Infrastructure, and Exit-Risk Failure
- Summary
- Evidence Supported
- Mechanism Identified
- Legal Frameworks Engaged
- Legal Duty
- Breach Identified
- Foreign-Controlled Infrastructure Risk
- Vendor Lock-In Risk
- Clinical Continuity Risk
- Data Portability and Record Integrity Risk
- Public-Law Risk
- Workforce Dependency Risk
- Patient Access Dependency Risk
- Tribunal / Procedural Risk
- Disclosure Questions
- Evidence Relied Upon
- Final Breach Position
- Consolidated Breach Conclusion — NHS AI Disclosure Position
- Summary
- Consolidated Breach Pattern
- Central Finding
- Core Public-Interest Statement
- Unified Legal Position
- Consolidated Disclosure Demands
- 1. Full AI System Register
- 2. Execution and Processing Map
- 3. Vendor and Sub-Processor Map
- 4. Clinical Safety Evidence
- 5. DPIA and Data Protection Evidence
- 6. Equality and Accessibility Evidence
- 7. Patient Consent and Objection Route
- 8. Staff Training and Liability Protection
- 9. AI Evidence Protocol
- 10. Sovereign Exit and Continuity Plan
- Consolidated Remedy Sought
- Final Disclosure Position
- Legal and Human Rights Frameworks Engaged
- Legal Frameworks Engaged.
- I.1 Magna Carta 1215 — Law of the Land / Protection Against Arbitrary Interference
- I.2 Magna Carta 1215 — Unsupported Official Assertion and Evidential Foundation
- I.3 Canon Law — Confessional Confidentiality and Protected Disclosure
- II. Common Law — Confidentiality and Privacy Layer
- II.2 Breach of Confidence
- II.3 Misuse of Private Information
- III.4 Human Rights Act 1998, Schedule 1, Article 6 — Right to a Fair Hearing
- III.5 Human Rights Act 1998, Schedule 1, Article 10 — Freedom of Expression
- III.6 Human Rights Act 1998, Schedule 1, Article 13 — Effective Remedy
- IV.8 Equality Act 2010, Section 29 — Services and Public Functions
- IV.9 Equality Act 2010, Section 149 — Public Sector Equality Duty
- V. NHS Constitution — Patient Rights, Confidentiality, and Safe Care Layer
- V.1 NHS Constitution — Privacy and Confidentiality
- V.2 NHS Constitution — Involvement in Healthcare Decisions
- V.3 NHS Constitution — Safe and Appropriate Care
- V.4 NHS Constitution — Dignity, Respect, and Compassionate Care
- V.5 NHS Constitution — Patient Choice and Access to Services
- V.6 NHS Constitution — Complaints, Redress, and Patient Voice
- V.7 NHS Constitution — Staff Responsibilities and Patient Confidentiality
- VI. Caldicott Principles — Medical Confidentiality Governance Layer
- VI.1 Caldicott Principle 1 — Justify the Purpose
- VI.2 Caldicott Principle 2 — Do Not Use Confidential Information Unless Necessary
- VI.3 Caldicott Principle 3 — Use the Minimum Necessary Confidential Information
- VI.4 Caldicott Principle 4 — Access on a Strict Need-to-Know Basis
- VI.5 Caldicott Principle 5 — Everyone Must Understand Their Responsibilities
- VI.6 Caldicott Principle 6 — Comply With the Law
- VI.7 Caldicott Principle 7 — Duty to Share Can Be as Important as Duty to Protect
- VI.8 Caldicott Principle 8 — Inform Patients and Service Users About How Their Confidential Information Is Used
- VII. UK GDPR and Data Protection Act 2018 — Statutory Data Protection Layer
- VII.1 UK GDPR Article 5 — Core Processing Principles
- VII.2 UK GDPR Article 6 — Lawful Basis for Processing
- VII.3 UK GDPR Article 9 — Special Category Health Data
- VII.4 UK GDPR Articles 13–14 — Transparency and Information Duties
- VII.5 UK GDPR Article 15 — Right of Access
- VII.6 UK GDPR Article 16 — Right to Rectification
- VII.7 UK GDPR Articles 17–18 — Erasure and Restriction of Processing
- VII.8 UK GDPR Article 21 — Right to Object
- VII.9 UK GDPR Article 22 — Automated Decision-Making and Profiling
- VII.10 UK GDPR Article 25 — Data Protection by Design and Default
- VII.11 UK GDPR Article 28 — Processor and Sub-Processor Controls
- VII.12 UK GDPR Article 30 — Records of Processing Activities
- VII.13 UK GDPR Article 32 — Security of Processing
- VII.14 UK GDPR Article 35 — Data Protection Impact Assessment
- VII.15 UK GDPR Articles 44–49 — International Transfers
- VII.16 Data Protection Act 2018 — Domestic Statutory Supplement to UK GDPR
- VII.17 Data Protection Act 2018 — Section 10 and Schedule 1, Special Category Processing Conditions
- VII.18 Data Protection Act 2018 — Schedule 1, Health or Social Care Purposes
- VII.19 Data Protection Act 2018 — Schedule 1, Public Health
- VII.20 Data Protection Act 2018 — Schedule 1, Research Purposes
- VII.21 Data Protection Act 2018, Section 170 — Unlawful Obtaining, Disclosure, or Retention of Personal Data
- VII.22 Data Protection Act 2018, Section 171 — Re-Identification of De-Identified Personal Data
- VII.23 Data Protection Act 2018, Section 173 — Alteration of Personal Data to Prevent Disclosure
- VII.24 UK GDPR Article 5(2) and Article 35 — Accountability Principle and Undetermined Extraterritorial Engagement
- VIII. Clinical Safety, Health IT, Medical Device, and Healthcare Records Governance Layer
- VIII.1 Health and Social Care Act 2012 — Information Standards and Clinical Safety Governance
- VIII.2 DCB0129 — Clinical Risk Management in Manufacture of Health IT Systems
- VIII.3 DCB0160 — Clinical Risk Management in Deployment and Use of Health IT Systems
- VIII.4 Digital Clinical Safety Assurance — Hazard Logs and Clinical Safety Cases
- VIII.5 Digital Technology Assessment Criteria — Clinical Safety, Data Protection, Security, Interoperability, Usability, and Accessibility
- VIII.6 UK Medical Device Regulations 2002 — Software With a Medical Purpose
- VIII.7 MHRA Software and AI as a Medical Device Guidance
- VIII.8 NICE Evidence Standards Framework for Digital Health Technologies
- VIII.9 Duty of Candour — Openness When Things Go Wrong
- VIII.10 NHS Records Management Code of Practice — AI-Derived Records and Retention
- VIII.11 Professional Duties — Accurate Clinical Records and Confidentiality
- IX. Employment, Whistleblowing, Staff Safety, and Workplace Protection Layer
- IX.1 Employment Rights Act 1996, Section 43B — Qualifying Disclosures
- IX.2 Employment Rights Act 1996, Section 47B — Protected Disclosure Detriment
- IX.3 Employment Rights Act 1996, Section 98 — Fairness in Dismissal
- IX.4 Employment Rights Act 1996, Section 103A — Protected Disclosure Dismissal
- IX.5 Public Interest Disclosure Act 1998 — Whistleblowing Protection Framework
- IX.6 Health and Safety at Work etc. Act 1974, Section 2 — Employer Duty to Employees
- IX.7 Management of Health and Safety at Work Regulations 1999 — Risk Assessment
- IX.8 HSE Management Standards — Work-Related Stress
- IX.9 ACAS Code of Practice — Disciplinary and Grievance Procedures
- IX.10 Common Law Implied Duty of Mutual Trust and Confidence
- IX.11 Employer Common Law Duty of Care
- XI.2 Evidential Reliability — Source-to-Output Traceability
- XI.3 Disclosure Duties — AI-Derived Material Must Be Disclosed Where Relevant
- XI.4 Preservation Duties — AI Records Must Not Be Lost, Overwritten, or Normalised
- XI.5 Authenticity and Metadata — AI Evidence Requires Provenance
- XI.6 Human Review — Meaningful Review Cannot Be Assumed
- XI.7 Automation Bias — AI Outputs May Be Over-Relied Upon
- XI.8 Litigation Prejudice — AI Systems May Create Hidden Material Relevant to Proceedings
- XI.9 Complaint Fairness — AI Involvement Must Be Visible in NHS Complaints
- XI.10 Tribunal Fairness — AI-Derived Employment Material Requires Disclosure and Challenge
- XI.11 Burden of Verification — AI Shifts Evidential Labour Onto Patients and Staff
- XI.12 Audit-Trail Fairness — Logs Are Not Neutral Evidence Unless Interpreted Correctly
- XII. International Human Rights, Privacy, Bioethics, and Business-Human-Rights Layer
- XII.1 Universal Declaration of Human Rights, Article 12 — Privacy, Family, Home, and Correspondence
- XII.2 Universal Declaration of Human Rights, Article 19 — Freedom to Seek, Receive, and Impart Information
- XII.3 International Covenant on Civil and Political Rights, Article 17 — Privacy Protection
- XII.4 International Covenant on Economic, Social and Cultural Rights, Article 12 — Right to the Highest Attainable Standard of Health
- XII.5 International Covenant on Economic, Social and Cultural Rights, Article 7 — Just and Favourable Conditions of Work
- XII.6 Council of Europe Convention 108+ — Data Protection, Dignity, and Fundamental Freedoms
- XII.7 OECD Privacy Guidelines — Collection Limitation, Purpose Specification, Use Limitation, Security, Openness, Participation, and Accountability
- XII.8 UNESCO Universal Declaration on Bioethics and Human Rights, Article 5 — Autonomy and Individual Responsibility
- XII.9 UNESCO Universal Declaration on Bioethics and Human Rights, Article 6 — Consent
- XII.10 UNESCO Universal Declaration on Bioethics and Human Rights, Article 9 — Privacy and Confidentiality
- XII.11 UNESCO Universal Declaration on Bioethics and Human Rights, Article 10 — Equality, Justice, and Equity
- XII.12 UNESCO Universal Declaration on Bioethics and Human Rights, Article 11 — Non-Discrimination and Non-Stigmatization
- XII.13 UNESCO Universal Declaration on Bioethics and Human Rights, Article 15 — Sharing of Benefits
- XII.14 UN Guiding Principles on Business and Human Rights — Corporate Responsibility to Respect Human Rights
- XII.15 Nuremberg Code — Voluntary Consent and Medical Experimentation Boundary
- Legal Frameworks Conclusion
- 1. Domestic legal foundations
- 2. Common law confidentiality and privacy
- 3. Human rights
- 4. Equality law
- 5. NHS-specific rights and confidentiality governance
- 6. Data protection law
- 7. Clinical safety, health IT, medical-device, and records governance
- 8. Staff, whistleblowing, and workplace protection
- 9. Public law, procurement, public money, continuity, and sovereignty
- 10. Evidential and procedural fairness
- 11. International human-rights, privacy, bioethics, and business-human-rights standards
- Disclosure Conclusion
- 1. The central issue
- 2. Patient-side consequence
- 3. Staff-side consequence
- 4. Clinical safety consequence
- 5. Equality consequence
- 6. Data protection and confidentiality consequence
- 7. Re-identification consequence
- 8. Evidential consequence
- 9. Procurement and sovereignty consequence
- 10. Required public proof
- 11. Final disclosure position
Executive Summary
This disclosure records a live public-interest concern arising from the concurrent deployment of artificial intelligence systems across NHS patient-access, workforce, administrative, triage, ambient voice, clinical-documentation, and data-processing environments.
The disclosure does not concern ordinary NHS digitisation.
It concerns the structural shift from human-administered healthcare access and clinical documentation into AI-mediated systems where patient symptoms, patient speech, staff inputs, clinical notes, appointment requests, administrative workflows, prompts, logs, telemetry, audit trails, and behavioural patterns may be processed through SaaS platforms, cloud infrastructure, proprietary models, automated triage engines, transcription systems, generative AI tools, and externally controlled processing chains.
The disclosure identifies a central distinction:
data storage is not data execution.
A statement that data is stored on servers in England or the United Kingdom does not answer the legal sovereignty question. The relevant question is where the data is processed, executed, modelled, inferred, classified, logged, analysed, monitored, debugged, audited, retained, used for system improvement, or exposed through support-access pathways.
This disclosure therefore concerns the point at which patient and worker data stops being passive information and becomes operational AI output.
The disclosure records that NHS AI triage, ambient voice technology, Microsoft Copilot-style workflow tools, SaaS clinical systems, cloud-hosted processing environments, AI transcription, automated routing, and model-generated summaries may each create distinct legal consequences.
Those consequences include:
- patient-access routing;
- urgency classification;
- appointment prioritisation;
- pharmacy / GP / A&E / self-care redirection;
- voice-to-text clinical capture;
- AI-generated clinical summaries;
- patient-record formation;
- staff audit trails;
- disciplinary exposure;
- employment liability;
- protected-disclosure detriment risk;
- tribunal / procedural reliance risk;
- identifiable medical-data exposure;
- pattern-based re-identification;
- and cross-border data-bleed risk.
This disclosure further records the contradiction created where NHS staff may be placed into AI-enabled systems while public communication warns of dismissal or imprisonment for improper record access. The issue is not whether patient records require protection. They plainly do. The issue is whether a national healthcare employer can deploy AI-mediated tools into live patient and staff environments, retain institutional control over licences, systems, permissions, procurement, audit, training, and escalation pathways, and then position individual workers as the visible endpoint of criminal, disciplinary, or reputational liability.
This is not ordinary confidentiality enforcement.
It is a workforce-governance and liability-displacement problem.
Scope of This Disclosure
This disclosure encompasses NHS AI deployment across the following connected operating environments:
1. Patient-access AI triage
AI or automated systems that receive patient symptom data and produce urgency, routing, appointment, pharmacy, GP, A&E, self-care, or clinician-prioritisation outputs.
2. Voice / speech-dependent AI pathways
AI systems that rely on spoken input, accent recognition, transcription, voice capture, patient speech, clinician speech, background-noise filtering, multi-speaker separation, or language interpretation.
3. Ambient voice technology
Systems that capture consultation speech and generate notes, summaries, letters, or structured content capable of entering the patient record.
4. Staff-facing AI workflow systems
AI tools deployed to NHS staff for administrative work, summarisation, drafting, email, scheduling, clinical-support documentation, productivity, or patient-related workflow assistance.
5. SaaS and cloud processing
Third-party platforms, cloud services, application layers, model engines, inference services, telemetry systems, sub-processors, support systems, backup routes, and analytics environments used to process NHS patient or workforce data.
6. Patient-record integrity
The risk that AI-generated, AI-transcribed, AI-summarised, or AI-routed information becomes part of the medical record or influences care pathways.
7. Workforce liability and tribunal consequence
The risk that AI logs, audit trails, generated outputs, system classifications, access histories, prompts, or automated records may later be relied upon in employment, disciplinary, tribunal, protected-disclosure, or procedural contexts.
Public-Interest Position
This disclosure is made in the public interest because NHS AI deployment affects both sides of the healthcare relationship:
patients, whose symptoms, voices, access routes, medical identities, and care pathways may be processed through AI systems; and
workers, whose actions, prompts, access patterns, errors, corrections, AI reliance, audit trails, and verification burdens may become disciplinary, employment, tribunal, or liability material.
The disclosure identifies not fewer than 18 breach categories and not fewer than 90 legal, regulatory, clinical-safety, equality, employment, tribunal, human-rights, data-protection, AI-governance, bioethical, and medical-sovereignty frameworks.
Each breach is to be addressed using the following structure:
mechanism → evidence supported → legal frameworks engaged → verbatim legal text → legal duty → breach identified → analysis → disclosure questions → evidence relied upon.
The purpose is not to assert a single isolated failure.
The purpose is to record the operating architecture through which multiple failures may arise simultaneously.
Core Structural Contradiction
The core contradiction is this:
NHS AI systems are being advanced as productivity, safety, access, and efficiency tools, while the public record does not visibly establish the execution architecture, processing model, clinical safety assurance, equality testing, voice / accent validation, patient-consent pathway, staff-liability boundary, or sovereign control structure required for lawful deployment at national scale.
That contradiction becomes sharper where public messaging threatens NHS staff with dismissal or imprisonment while the systems themselves introduce new ambiguity into:
- who accessed what;
- who processed what;
- who relied on what;
- who verified what;
- what AI generated;
- what the model inferred;
- what was logged;
- what was retained;
- what crossed systems;
- what entered the medical record;
- and who becomes responsible when AI output is wrong.
The disclosure therefore distinguishes between:
human misconduct
and
system-created liability exposure.
The former may be dealt with through ordinary disciplinary, confidentiality, criminal, or regulatory pathways.
The latter requires scrutiny of the employer, the system owner, the processor, the vendor, the cloud provider, the model operator, the deployment authority, and the public body responsible for ensuring lawful, safe, fair, transparent, and accountable use.
Central Thesis
The central thesis of this disclosure is:
NHS AI deployment creates a national processing architecture in which patient data, staff data, voice data, symptom data, clinical context, behavioural access patterns, audit logs, and AI outputs may be converted into healthcare decisions, employment consequences, patient-record entries, and legal evidence before the public has been shown where the data is executed, how the model operates, who controls the processing chain, whether patients meaningfully consent, whether staff are protected, whether accents and language variation have been validated, whether clinical safety standards have been satisfied, and whether sovereign exit from foreign-controlled AI infrastructure is possible.
This is why the disclosure cannot be confined to data protection alone.
It engages:
- medical confidentiality;
- AI governance;
- public law;
- equality law;
- clinical safety;
- employment law;
- tribunal fairness;
- whistleblowing detriment;
- human rights;
- cybersecurity;
- cloud dependency;
- international data-transfer risk;
- bioethics;
- consent;
- and public-sector accountability.
Disclosure Position
This disclosure does not allege that every NHS AI use is unlawful.
It records that the legal safety of NHS AI deployment cannot be assessed from headline claims, pilot summaries, storage-location statements, productivity estimates, or broad assurances.
The required evidence is the processing map.
That map must identify:
- the AI system;
- the vendor;
- the model;
- the processing engine;
- the execution location;
- the cloud service;
- the sub-processors;
- the support-access pathway;
- the telemetry pathway;
- the logging pathway;
- the backup and disaster-recovery pathway;
- the model-improvement pathway;
- the clinical safety case;
- the equality assessment;
- the DPIA;
- the patient-consent wording;
- the staff-training framework;
- the accent / dialect / language validation evidence;
- the human-review point;
- the correction route;
- the appeal route;
- the audit route;
- and the liability route.
Without that map, NHS AI deployment remains jurisdictionally, clinically, procedurally, and legally unresolved.
Working Breach Set
This disclosure proceeds by breach.
The current breach set is:
- Public Criminal-Threat Governance and Staff Liability Displacement
- Mass Named-User AI Licence Exposure and Audit-Trail Liability
- AI Triage Processing Sovereignty and Undisclosed Decision Engine
- Data Execution, Modelling Location, and Cross-Border Data-Bleed Non-Disclosure
- AI Triage Output Traceability, Accuracy, and Human-Review Failure
- Voice / Speech AI Accent Validation Failure and Unsafe National Scaling from Sussex Pilot Evidence
- Ambient Voice Technology and AI-Mediated Clinical Record Formation
- Patient Consent, Transparency, and Meaningful Choice Failure
- Pseudonymisation, Re-Identification, and Pattern-Correlation Failure
- Staff Digital Competence, Training, and Professionalisation Mismatch
- Clinical Safety Case, DPIA, Equality Impact, and Assurance Visibility Failure
- Patient Access Inequality and Digital Exclusion
- Cybersecurity Blind Spot: Authorised Use as Exposure Pathway
- AI Hallucination, Verification Burden, and Workforce Stress Risk
- Vendor, Sub-Processor, Cloud, Telemetry, and Support-Access Disclosure Failure
- Accountability Gap Between NHS England, ICBs, GP Practices, Vendors, and Staff
- AI Output Reliance in Employment, Disciplinary, Tribunal, and Protected-Disclosure Contexts
- Public-Sector AI Dependency, Foreign-Controlled Infrastructure, and Exit-Risk Failure
Opening Conclusion
This disclosure records NHS AI deployment as a national legal-governance event, not a technology upgrade.
The issue is no longer whether AI can assist healthcare.
The issue is whether AI is being inserted into patient access, clinical speech, medical records, workforce audit, staff discipline, cloud infrastructure, SaaS processing, and public-sector dependency before the necessary legal architecture has been disclosed.
The breach pattern is therefore clear:
deployment precedes proof; storage statements replace execution disclosure; pilot evidence is treated as national validation; AI output enters patient and worker pathways; staff are threatened before liability is settled; and patient sovereignty is reduced to infrastructure assurance rather than processing truth.
Core line:
The breach is not where the data rests. The breach is where the data acts.
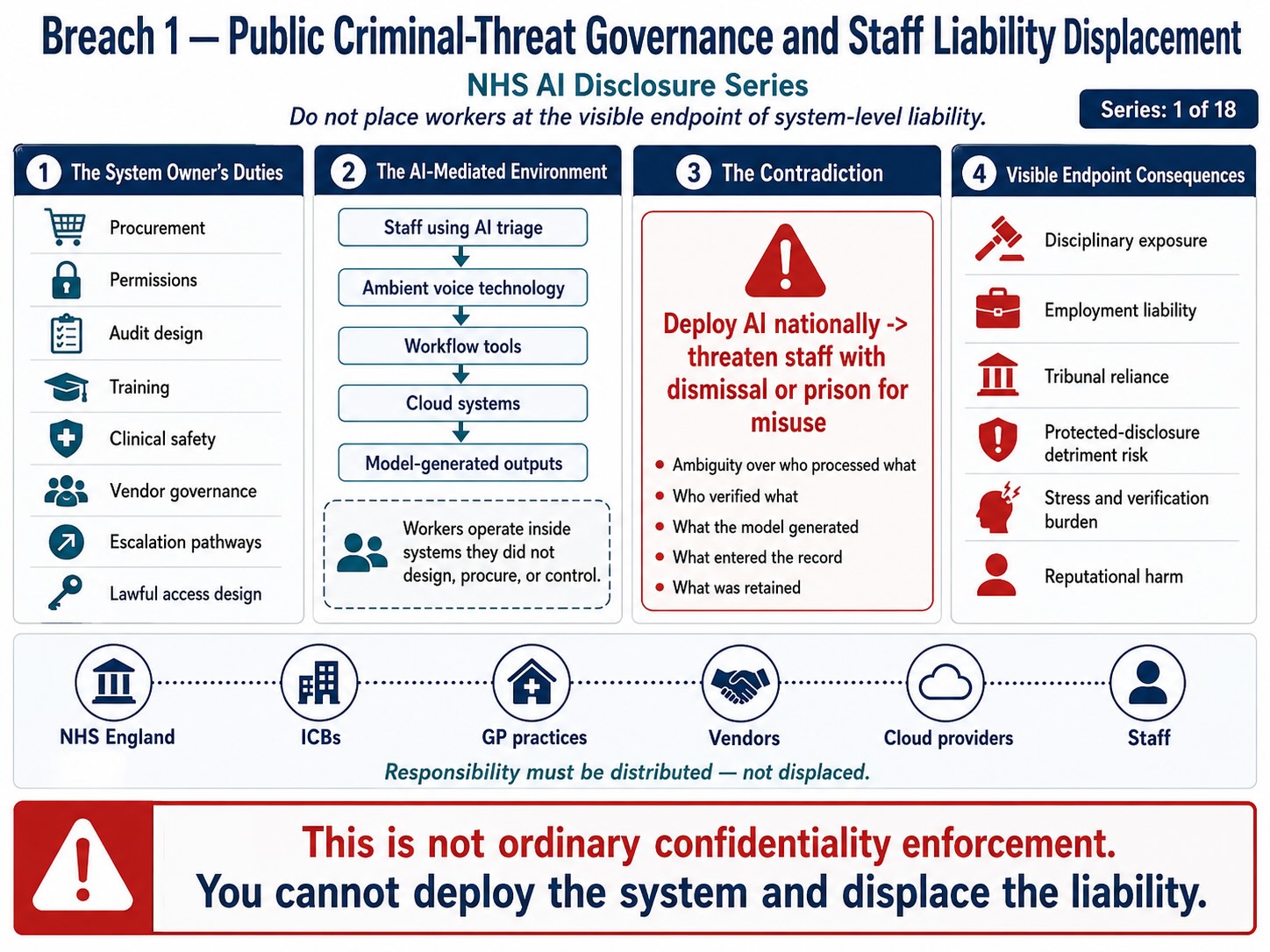
Figure 1 : Breach 1 — Public Criminal-Threat Governance and Staff Liability Displacement. This figure shows how NHS AI deployment can place workers at the visible endpoint of liability while system owners retain control over procurement, permissions, audit design, training, clinical safety, vendor governance, escalation pathways, and lawful access architecture. The breach is the displacement of institutional responsibility onto staff before the AI-mediated processing chain is transparently governed.
Breach I — Public Criminal-Threat Governance and Staff Liability Displacement
Summary
This breach concerns the public issuing of criminal-threat language toward NHS staff at the same time as NHS England is expanding AI-enabled systems across staff workflows, patient-access pathways, clinical documentation, ambient voice technology, and administrative environments.
The issue is not whether NHS staff should be prevented from improperly accessing patient records.
They should.
The breach concerns the governance sequence.
NHS England controls or materially influences the deployment architecture:
- procurement;
- licences;
- access permissions;
- role configuration;
- acceptable-use policies;
- audit systems;
- AI tools;
- staff training;
- data-governance rules;
- disciplinary escalation;
- and public communication.
Yet the public message places the visible liability endpoint on the individual worker through language of dismissal and prison before the AI-processing, staff-competence, patient-consent, audit, verification, and liability boundaries are visibly settled.
The breach is therefore:
institutional deployment → system control retained by employer → AI-enabled ambiguity introduced → public criminal-threat language directed at staff → individual worker positioned as liability endpoint.
Evidence Supported
NHS England published a public warning stating that staff may face dismissal or prison if they access patient records without a legitimate reason. The announcement describes a crackdown on inappropriate access to patient data and frames the consequence in disciplinary and criminal terms. (NHS England)
This warning sits beside NHS England’s wider AI deployment programme. NHS England announced that more than 500,000 NHS staff would receive Microsoft 365 Copilot after a trial involving more than 30,000 NHS workers across 90 NHS organisations, with claimed average administrative time savings of 43 minutes per staff member per day. (NHS England)
NHS England has also backed ambient voice technologies, describing them as systems that capture clinician–patient conversations and use AI to generate real-time transcriptions and clinical summaries. (NHS England)
Separately, NHS AI triage is being advanced through the NHS App, with public reporting describing triage outputs that may route patients toward GP appointments, pharmacies, A&E, or other services. (The Guardian)
Together, these sources support the breach mechanism:
staff-facing AI tools + patient-access AI triage + ambient voice clinical capture + patient-record enforcement warning = widened worker-liability surface.
Mechanism Identified
The operating mechanism is:
NHS staff account → named AI licence / system access → patient-adjacent workflow → AI assistance / prompt / summary / transcription / triage / record access → audit log → employer review → disciplinary or criminal escalation risk
This mechanism creates a new liability surface because AI systems may generate, summarise, recommend, classify, retrieve, or display information in ways that staff must verify.
The worker may be judged later against an audit trail created inside an AI-enabled environment that the worker did not design, procure, configure, or govern.
That creates liability displacement.
Legal Frameworks Engaged
This breach engages, at minimum:
- Health and Safety at Work etc. Act 1974, section 2 — employer duty to provide a safe system of work.
- Management of Health and Safety at Work Regulations 1999 — workplace risk assessment.
- Employment Rights Act 1996, section 98 — fairness in dismissal.
- Employment Rights Act 1996, section 47B — detriment for protected disclosure, where staff challenge unsafe AI/data practice.
- Employment Rights Act 1996, section 103A — automatic unfair dismissal for protected disclosure.
- Public Interest Disclosure Act 1998 — protection for qualifying disclosures.
- ACAS Code of Practice on Disciplinary and Grievance Procedures — fair process before disciplinary sanction.
- Common law implied duty of mutual trust and confidence — employer must not act without reasonable and proper cause in a way likely to destroy trust.
- Employer common law duty of care — foreseeable psychiatric or occupational harm.
- Equality Act 2010 — where threat, training gap, AI literacy, disability, race, language, nationality, or accent-related disadvantage is engaged.
- Equality Act 2010, section 149 — Public Sector Equality Duty.
- Human Rights Act 1998 / ECHR Article 8 — private life, dignity, reputation, psychological integrity.
- Human Rights Act 1998 / ECHR Article 6 — fair process where disciplinary or tribunal reliance arises.
- Natural justice — right to know the case, answer the case, and have evidence fairly assessed.
- Employment Tribunal Rules / overriding objective — fair and just handling of proceedings where AI logs or outputs are later relied upon.
- UK GDPR Article 5(1)(a) — lawful, fair, transparent processing of staff and patient data.
- UK GDPR Article 5(1)(d) — accuracy of data relied on in audit or disciplinary context.
- UK GDPR Article 15 — staff/patient right of access to data relied upon.
- UK GDPR Article 16 — rectification of inaccurate data.
- UK GDPR Article 22 — automated decision-making / profiling, where automated outputs materially affect staff or patients.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 35 — DPIA for high-risk processing.
- EU AI Act Article 13 — transparency and information sufficient to interpret output.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness, and cybersecurity.
- EU AI Act Article 26 — deployer obligations, where applicable.
- UN Guiding Principles on Business and Human Rights — avoid causing or contributing to adverse human-rights impacts through business systems.
Legal Duty
NHS England and deploying NHS bodies must ensure that staff are not placed into AI-enabled systems where the boundaries of lawful use, prohibited use, patient-data handling, AI verification, audit interpretation, disciplinary reliance, and liability escalation are unclear.
Where a public employer deploys systems that create audit trails, AI-generated outputs, automated summaries, transcription records, triage recommendations, prompt histories, or patient-access logs, the employer must ensure that staff understand:
- what the system does;
- what data it accesses;
- what staff may input;
- what staff must not input;
- what AI output may be relied upon;
- what must be independently verified;
- what is logged;
- how logs may be used;
- how mistakes are corrected;
- how staff can challenge inaccurate AI-generated records;
- and when conduct becomes disciplinary or criminal.
Threat language cannot lawfully substitute for governance architecture.
Breach Identified
The breach identified is the apparent inversion of proper governance order.
The proper order is:
risk assessment → policy → training → role boundaries → AI literacy → patient-data safeguards → audit rules → human-review standards → disciplinary rules → enforcement
The apparent public sequence is:
AI deployment → mass staff access → productivity claim → ambient voice / triage expansion → public sack/prison warning → unresolved processing and liability questions
That creates a workforce liability-displacement architecture.
The staff member becomes the visible endpoint for a system they did not create.
The institution retains control of procurement, licence allocation, configuration, model selection, audit design, training design, data governance, and escalation policy, but the public warning foregrounds individual punishment.
That is the structural breach.
Tribunal / Procedural Risk
This breach also engages tribunal and procedural fairness because AI-generated records, access logs, prompts, summaries, triage outputs, transcription records, or audit events may later be relied upon in:
- disciplinary proceedings;
- dismissal decisions;
- professional-regulation referrals;
- employment tribunal claims;
- protected-disclosure detriment claims;
- unfair-dismissal proceedings;
- whistleblowing disputes;
- disability / equality claims;
- or credibility assessments.
Where AI-generated or AI-mediated material is used as evidence, the tribunal-facing questions become:
- was the output human-generated, AI-generated, or hybrid;
- was the audit trail complete;
- was the AI output accurate;
- was the worker trained;
- was the worker warned;
- was the system explainable;
- was the staff member able to challenge the data;
- was the underlying model disclosed;
- was the processing pathway disclosed;
- and was reliance on the output procedurally fair?
Disclosure Questions
- What staff roles are covered by the public sack/prison warning?
- Does the warning apply to staff using AI-enabled tools?
- Has NHS England distinguished between deliberate record snooping and AI-mediated workflow exposure?
- What AI systems generate audit trails capable of being used in staff investigations?
- Are Copilot prompts, summaries, document interactions, and retrieval histories logged?
- Are ambient voice transcripts and summaries linked to named staff users?
- Are AI triage overrides linked to named staff users?
- Can staff access, challenge, correct, or explain AI-generated audit material?
- What training was completed before staff were exposed to AI workflow tools?
- What policy defines permissible AI use involving patient data?
- What policy defines prohibited AI use?
- What policy defines when AI misuse becomes disciplinary misconduct?
- What policy defines when conduct becomes criminal referral?
- What safeguards distinguish human misconduct from system-created error?
- What safeguards distinguish deliberate access from AI-assisted retrieval, summarisation, or workflow exposure?
- What legal advice was taken before public criminal-threat language was issued?
- What occupational stress assessment was completed before issuing national threat messaging to NHS staff?
- What equality impact assessment was completed for staff with lower AI literacy, disabilities, language barriers, neurodivergence, or internationally trained backgrounds?
- What tribunal disclosure process will apply where AI logs are relied upon in employment litigation?
- What redress route exists where AI-generated material contributes to a false disciplinary allegation?
Evidence Relied Upon
EX-B1-01 — NHS England public warning that staff face dismissal or prison for inappropriate access to patient records. (NHS England)
EX-B1-02 — NHS England announcement of Microsoft 365 Copilot rollout to more than 500,000 staff, following 30,000-worker trial across 90 organisations and 43-minute productivity claim. (NHS England)
EX-B1-03 — Microsoft statement confirming NHS England acceleration of Microsoft 365 Copilot following initial NHS trial. (Source)
EX-B1-04 — NHS England ambient voice technology announcement describing AI systems that capture clinician–patient conversations and generate transcriptions / clinical summaries. (NHS England)
EX-B1-05 — Public reporting on NHS App AI triage routing patients to GP, pharmacy, A&E or other services. (The Guardian)
Final Breach Position
This breach records that NHS England has publicly warned staff of dismissal or imprisonment for improper patient-record access while simultaneously advancing AI systems that expand the complexity of patient-data access, workflow processing, audit trails, clinical documentation, and automated output reliance.
The breach is not confidentiality enforcement.
The breach is criminal-threat governance before AI liability settlement.
Core line:
NHS England cannot lawfully expand AI-mediated patient-data systems and then treat the individual worker as the criminal endpoint without first disclosing the training, audit, verification, processing, and liability architecture that governs the system.
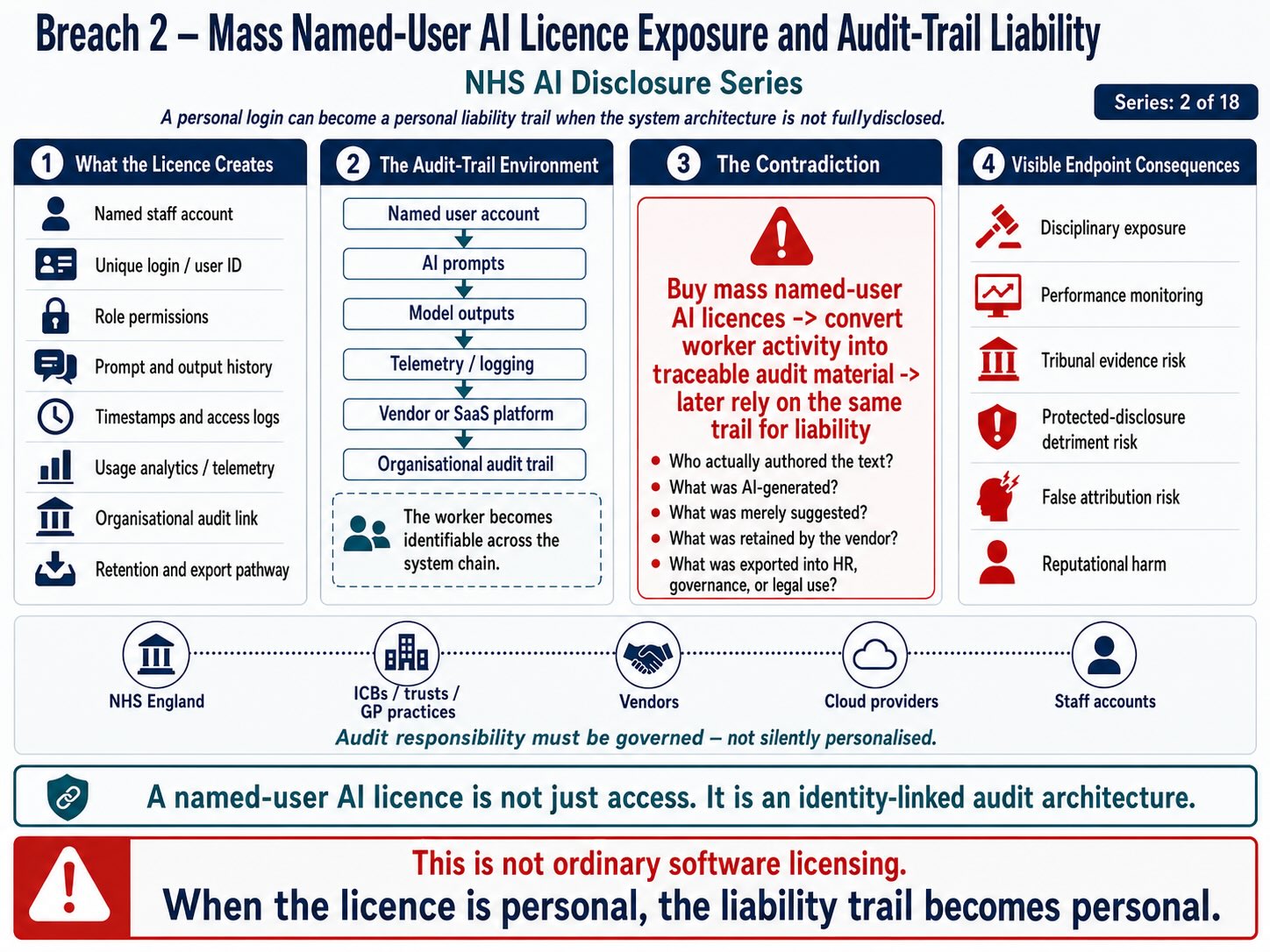
Figure 2: Breach 2 — Mass Named-User AI Licence Exposure and Audit-Trail Liability. This figure shows how personal AI licences can convert staff activity into identity-linked audit material through named accounts, prompts, outputs, telemetry, timestamps, vendor logs, and organisational audit trails. The breach is the creation of personal liability exposure before the system architecture, data-retention pathway, vendor access, and lawful use of audit material are fully disclosed.
Breach II — Mass Named-User AI Licence Exposure and Audit-Trail Liability
Summary
This breach concerns the mass allocation of AI-enabled licences to NHS staff, creating named-user exposure across administrative, clinical-support, patient-adjacent, workflow, document, communication, summarisation, and audit environments.
The breach is not simply that NHS staff are receiving AI tools.
The breach is that named AI access creates attributable records of worker conduct inside systems where prompts, document interactions, summaries, email drafts, retrieval events, audit logs, telemetry, access histories, and AI-assisted outputs may later be attributed to individual workers.
That creates a liability surface.
The worker becomes identifiable at the point of use, while the employer, vendor, processor, model operator, cloud provider, and deployment authority remain structurally upstream.
The breach mechanism is:
named staff licence → AI-assisted workflow → prompt / action / retrieval / output / edit / summary / access event → audit trail → employer review → disciplinary, regulatory, tribunal, or criminal exposure
Evidence Supported
NHS England announced that more than 500,000 NHS staff would receive Microsoft 365 Copilot access after a trial involving more than 30,000 NHS workers across 90 NHS organisations. NHS England reported an average administrative saving of 43 minutes per staff member per day. (NHS England)
Microsoft’s own public statement describes NHS England’s deployment of Microsoft 365 Copilot as a major AI adoption programme intended to improve service delivery, reduce costs, and create more time for care. (Source)
NHS England also issued a public warning that staff may face dismissal or prison if they access patient records without a legitimate reason. (NHS England)
Those facts create the supported disclosure pathway:
mass AI licences + named NHS staff users + patient-adjacent administrative tools + audit capability + public disciplinary/criminal threat language = expanded staff liability surface.
Mechanism Identified
The mechanism is not abstract.
A named NHS user logs into an AI-enabled Microsoft environment. The user may ask the AI to summarise, draft, search, restructure, analyse, retrieve, classify, translate, rewrite, compare, prioritise, or generate content connected to NHS work.
That may involve:
- patient-adjacent documents;
- emails;
- meeting notes;
- referral correspondence;
- policy documents;
- operational records;
- HR records;
- rota information;
- complaint material;
- triage material;
- clinical-administration notes;
- and workflow summaries.
Each interaction may create or interact with:
- user identity;
- time stamp;
- prompt text;
- document reference;
- retrieval event;
- generated output;
- edit history;
- audit log;
- usage analytics;
- security event;
- telemetry;
- retention record;
- and compliance review pathway.
That creates a worker-identifiable AI trace.
The governance issue is whether staff have been told clearly:
what is logged, what is retained, what is reviewed, who can see it, how it may be used, whether it may be used in discipline, and how inaccurate AI-generated or AI-linked records can be challenged.
Legal Frameworks Engaged
This breach engages, at minimum:
- UK GDPR Article 5(1)(a) — lawfulness, fairness, and transparency.
- UK GDPR Article 5(1)(b) — purpose limitation.
- UK GDPR Article 5(1)(c) — data minimisation.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(e) — storage limitation.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 6 — lawful basis for processing staff and patient data.
- UK GDPR Article 9 — special-category health data where patient-related material is processed.
- UK GDPR Article 13 — staff information where personal data is collected from them.
- UK GDPR Article 14 — information where personal data is generated or obtained indirectly.
- UK GDPR Article 15 — right of access to data held about the worker or patient.
- UK GDPR Article 16 — rectification of inaccurate personal data.
- UK GDPR Article 18 — restriction of processing.
- UK GDPR Article 21 — right to object.
- UK GDPR Article 22 — automated decision-making / profiling where AI-derived material materially affects the worker or patient.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 28 — processor obligations.
- UK GDPR Article 30 — records of processing activities.
- UK GDPR Article 32 — security of processing.
- UK GDPR Article 35 — DPIA for high-risk processing.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality where patient data is involved.
- Caldicott Principles.
- NHS Constitution — privacy, confidentiality, dignity, safe care.
- Health and Safety at Work etc. Act 1974 section 2 — safe system of work.
- Management of Health and Safety at Work Regulations 1999 — risk assessment.
- Employment Rights Act 1996 section 98 — fairness in dismissal.
- Employment Rights Act 1996 section 47B — detriment for protected disclosure.
- Employment Rights Act 1996 section 103A — automatic unfair dismissal for protected disclosure.
- Public Interest Disclosure Act 1998.
- ACAS Code of Practice on Disciplinary and Grievance Procedures.
- Common law implied duty of mutual trust and confidence.
- Equality Act 2010 where AI literacy, disability, language, race/national origin, age, or digital competence disparities affect staff exposure.
- Equality Act 2010 section 149 — Public Sector Equality Duty.
- Human Rights Act 1998 / ECHR Article 8 — dignity, reputation, private life, psychological integrity.
- Human Rights Act 1998 / ECHR Article 6 — fair process where AI logs or outputs are relied upon.
- Natural justice — right to know and answer the case.
- Employment Tribunal Rules / overriding objective — fair and just handling of proceedings.
- EU AI Act Article 13 — transparency and provision of information.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness, cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- EU AI Act Article 50 — transparency where AI interaction or generated output is relevant.
- UN Guiding Principles on Business and Human Rights — avoid adverse human-rights impacts through business systems.
Legal Duty
NHS England and deploying NHS bodies must ensure that staff-facing AI systems are introduced with clear, prior, role-specific governance.
That duty includes telling staff:
- what AI systems they are licensed to use;
- what data those systems can access;
- what data staff may input;
- what data staff must not input;
- whether prompts are retained;
- whether prompts are reviewed;
- whether generated outputs are retained;
- whether document references are logged;
- whether usage analytics identify individuals;
- whether AI telemetry is linked to named users;
- whether audit logs can be used in disciplinary proceedings;
- whether AI outputs may be relied upon as evidence;
- how errors can be corrected;
- how staff can challenge logs or generated records;
- and how human oversight is applied.
A public-sector employer cannot create a mass named-user AI audit environment while leaving the worker unclear about the evidential consequences of their AI use.
Breach Identified
The breach identified is the creation of a national named-user AI exposure system without visible settlement of staff-facing audit, liability, training, correction, access, retention, and disciplinary-use boundaries.
The deployment creates individualised traceability.
That traceability may be operationally useful.
But it is also legally dangerous if not governed.
The worker may later be judged by:
· what the AI system recorded;
· what the AI system retrieved;
· what the AI system generated;
· what the audit log shows;
· what the employer says the prompt meant;
· what the worker failed to correct;
· or what the system appears to show.
If the staff member cannot inspect, understand, challenge, contextualise, or correct that AI-linked record, the audit trail becomes a liability instrument.
That is the breach.
Tribunal / Procedural Risk
This breach directly engages tribunal and procedural law because AI audit trails may become evidence in employment disputes.
Possible use cases include:
- alleged misconduct;
- alleged inappropriate access;
- alleged breach of confidentiality;
- alleged failure to follow AI policy;
- alleged misuse of patient data;
- alleged negligence;
- protected-disclosure detriment;
- whistleblowing dismissal;
- disability or equality discrimination;
- capability/performance proceedings;
- and credibility disputes.
The tribunal risk is:
AI logs become evidence before the AI evidence chain is explained.
Procedural fairness requires disclosure of:
- the raw log;
- the system that created it;
- the time zone and timestamp logic;
- the retention policy;
- the identity-mapping process;
- whether the event was user-initiated or system-generated;
- whether AI retrieval occurred automatically;
- whether a generated output was accepted, edited, rejected, or ignored;
- whether the worker saw the final output;
- whether another user or administrator accessed the same material;
- whether the system produced hallucinated or inaccurate output;
- and whether the worker had training on that function.
Without that chain, the AI audit record is not procedurally safe.
Disclosure Questions
- How many NHS staff have been allocated named AI licences?
- Which staff groups are included?
- Which systems generate named-user AI logs?
- Are Copilot prompts retained?
- Are generated outputs retained?
- Are document references, retrieval events, or summarisation events retained?
- Are staff usage analytics linked to individual users?
- Are audit logs accessible to managers, HR, information governance teams, security teams, vendors, or Microsoft?
- Can AI logs be used in disciplinary investigations?
- Can AI outputs be used as evidence in employment tribunal proceedings?
- What training was provided before licence activation?
- What acceptable-use policy was issued before licence activation?
- What patient-data restrictions were given to staff?
- What safeguards distinguish deliberate access from AI-assisted retrieval?
- What safeguards distinguish staff instruction from automated system behaviour?
- Can staff obtain a copy of their AI usage data?
- Can staff challenge inaccurate usage records?
- Can staff correct AI-generated records attributed to them?
- Are AI logs retained after employment ends?
- Are AI logs shared with vendors or sub-processors?
- Are logs or telemetry processed outside the UK?
- Are prompts or outputs used for model improvement?
- What DPIA covers named staff AI usage?
- What equality assessment covers staff AI literacy and digital competence?
- What tribunal disclosure protocol applies where AI logs are relied upon?
Evidence Relied Upon
EX-B2-01 — NHS England announcement that more than 500,000 NHS staff will receive Microsoft 365 Copilot access after a trial involving more than 30,000 workers across 90 NHS organisations. (NHS England)
EX-B2-02 — Microsoft public statement on NHS England’s deployment of Microsoft 365 Copilot to improve service delivery, reduce costs, and create more time for care. (Source)
EX-B2-03 — NHS England public warning that staff may face dismissal or prison for inappropriate patient-record access. (NHS England)
Final Breach Position
This breach records that mass named-user AI licensing creates a national staff-identifiable audit environment.
The risk is not merely AI use.
The risk is AI use becoming evidence against the worker before the system’s logging, retention, accuracy, correction, disclosure, training, and liability architecture has been made clear.
Core line:
A named AI licence is not just a productivity tool. It is a worker-identifiable evidential surface.
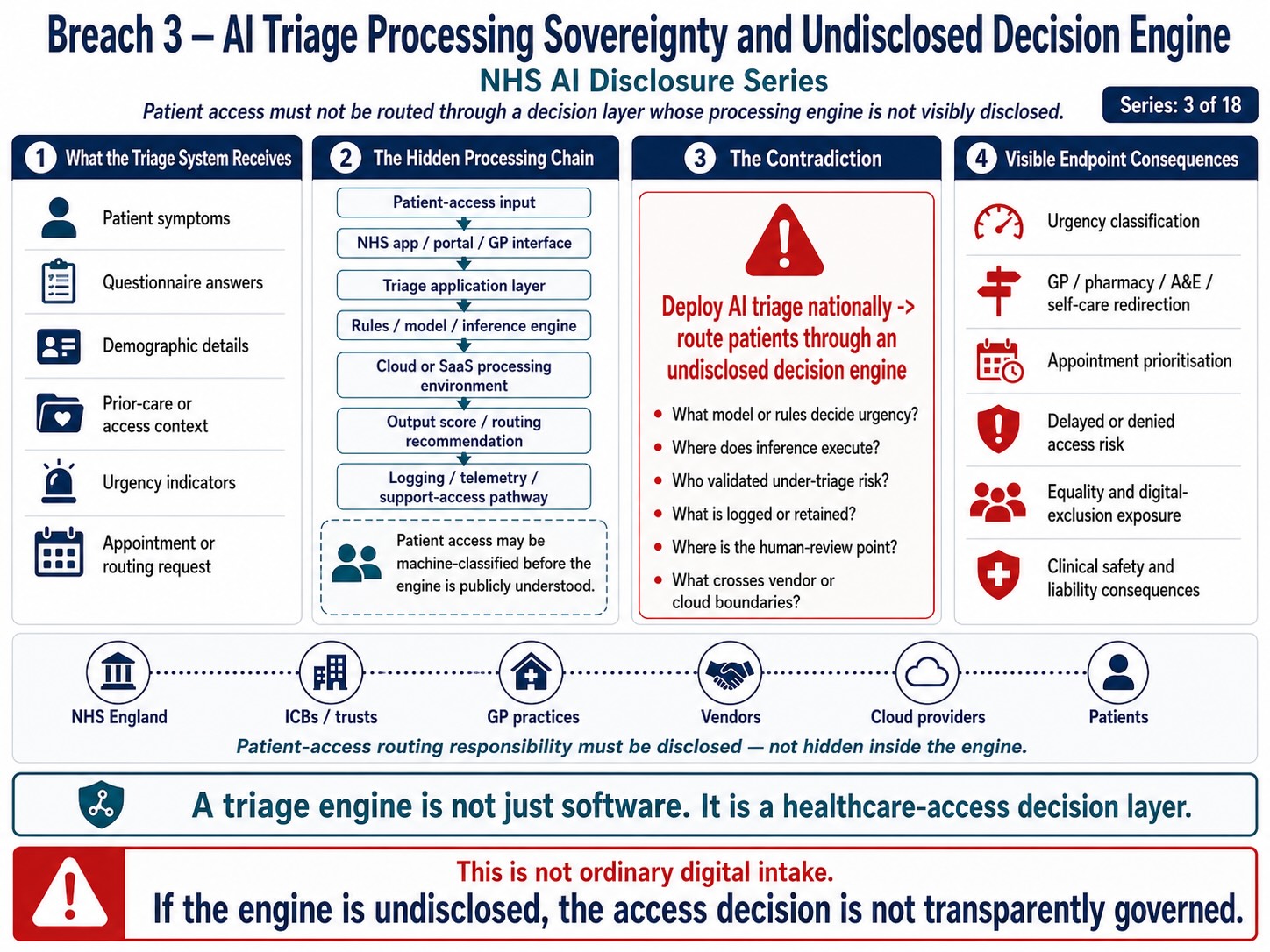
Breach 3 — AI Triage Processing Sovereignty and Undisclosed Decision Engine. This figure shows how AI triage can route patient access through a hidden processing chain involving intake interfaces, triage application layers, rules or inference engines, cloud or SaaS environments, output scoring, and logging pathways before the public can see how urgency, routing, and prioritisation decisions are made. The breach is the use of an undisclosed decision engine to influence access to care before the model logic, execution environment, human-review point, validation basis, and accountability chain are transparently disclosed.
Breach III — AI Triage Processing Sovereignty and Undisclosed Decision Engine
Summary
This breach concerns NHS AI triage systems where patient symptom data is submitted into an AI / automated triage pathway and converted into urgency, routing, appointment, pharmacy, GP, A&E, self-care, or clinician-prioritisation outputs.
The breach is not answered by saying the data is stored in England or the United Kingdom.
That answers storage.
It does not answer processing.
The sovereignty question is:
What executes the data?
The public record must identify the computational engine that receives patient symptom input and turns it into healthcare-access output.
That may include:
- rules engine;
- clinical protocol engine;
- machine-learning classifier;
- large language model;
- proprietary triage model;
- managed AI service;
- cloud inference service;
- decision-tree engine;
- risk-scoring model;
- ranking system;
- appointment-routing algorithm;
- or hybrid model.
Until that processing engine is disclosed, NHS AI triage remains a jurisdictionally unresolved patient-access system.
The breach mechanism is:
patient symptom disclosure → AI / SaaS triage interface → undisclosed processing engine → urgency / routing output → appointment or service pathway → patient access consequence
Evidence Supported
NHS England has publicly announced AI triage as part of NHS App expansion, describing a system intended to direct patients to the most appropriate NHS service.
Public reporting describes the NHS App AI triage pathway as routing patients toward GP appointments, pharmacy, A&E, or other services, with rollout following local trial evidence.
Rapid Health publicly describes Smart Triage as an autonomous AI triage and booking system operating within clinician-defined protocols.
The NHS Innovation Accelerator describes Smart Triage as a fully autonomous AI-powered triage and appointment booking system integrated with EMIS and TPP SystmOne, reducing manual data entry and staff intervention.
Those sources support the operational pathway:
patient input → automated / AI triage system → clinical protocol or AI processing layer → triage classification → appointment / routing output → GP workflow integration
That is not passive data storage.
That is patient-access processing.
Mechanism Identified
The mechanism is:
patient enters symptom data → system collects medical context → system processes input → system applies triage logic → system produces urgency or routing output → system may book, redirect, prioritise, or escalate → output enters GP / NHS workflow
The legal issue sits in the middle of that chain:
system processes input → system applies triage logic → system produces output
That is the point where sovereignty, explainability, accuracy, accountability, and liability attach.
A storage notice may say where the patient request is held.
It does not establish:
- where inference runs;
- what model performs classification;
- whether the model is rules-based, ML-based, LLM-based, or hybrid;
- whether a third-party AI service is used;
- whether processing is confined to the UK;
- whether telemetry leaves the UK;
- whether support staff can access processing logs;
- whether system behaviour is analysed elsewhere;
- whether symptom patterns are used to improve the product;
- whether the model can be audited;
- whether the patient can challenge the output;
- or whether a clinician reviews the output before any routing consequence.
This is the breach.
Legal Frameworks Engaged
This breach engages, at minimum:
- UK GDPR Article 5(1)(a) — lawfulness, fairness, and transparency.
- UK GDPR Article 5(1)(b) — purpose limitation.
- UK GDPR Article 5(1)(c) — data minimisation.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 6 — lawful basis for processing.
- UK GDPR Article 9 — special-category health data.
- UK GDPR Article 13 — information to be provided to the data subject.
- UK GDPR Article 15 — right of access.
- UK GDPR Article 16 — rectification.
- UK GDPR Article 21 — right to object.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 28 — processor obligations.
- UK GDPR Article 30 — records of processing activities.
- UK GDPR Article 32 — security of processing.
- UK GDPR Article 35 — Data Protection Impact Assessment.
- UK GDPR Articles 44–49 — international transfers, where non-UK processing or access exists.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality.
- Caldicott Principles.
- NHS Constitution — privacy, confidentiality, informed involvement and safe care.
- Human Rights Act 1998 / ECHR Article 8 — medical privacy, bodily autonomy and private life.
- Human Rights Act 1998 / ECHR Article 14 — non-discrimination in access to healthcare rights.
- Equality Act 2010 section 29 — services and public functions.
- Equality Act 2010 section 149 — Public Sector Equality Duty.
- Common law negligence / duty of care — foreseeable harm from wrong triage or misrouting.
- Public law rationality and proportionality — deployment must be evidence-based and proportionate.
- DCB0129 / DCB0160 clinical safety standards where clinical software affects patient pathways.
- EU AI Act Article 9 — risk management system.
- EU AI Act Article 10 — data and data governance.
- EU AI Act Article 11 — technical documentation.
- EU AI Act Article 12 — record keeping / logs.
- EU AI Act Article 13 — transparency and provision of information.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness and cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- EU AI Act Article 50 — AI interaction / AI-generated output transparency where applicable.
- UNESCO Bioethics Article 5 — autonomy and individual responsibility.
- UNESCO Bioethics Article 6 — consent.
- UNESCO Bioethics Article 9 — privacy and confidentiality.
- UNESCO Bioethics Article 10 — equality, justice and equity.
- ICCPR Article 17 — privacy.
- ICESCR Article 12 — right to health.
- UN Guiding Principles on Business and Human Rights — corporate responsibility to avoid adverse human-rights impacts.
Legal Duty
NHS England, ICBs, GP practices, and vendors deploying AI triage must disclose and govern the full processing chain, not merely the storage location.
The duty includes:
- identifying the AI / automation system;
- identifying the processing engine;
- identifying whether the system is rules-based, ML-based, LLM-based, or hybrid;
- identifying where inference occurs;
- identifying whether any managed AI service is used;
- identifying all processors and sub-processors;
- identifying where logs, telemetry, analytics, and model-monitoring data are processed;
- identifying whether patient symptom data is used for product improvement;
- identifying how triage output is validated;
- identifying how human oversight operates;
- identifying how patients can challenge or correct output;
- and identifying the liability chain where routing is wrong.
A healthcare access system cannot lawfully rely on opaque processing where the output may affect patient access, urgency, care route, or delay.
Breach Identified
The breach identified is the apparent absence of visible public disclosure identifying the decision engine and execution pathway behind NHS AI triage.
The public record may describe triage benefits, patient routing, integration, and storage assurances.
But the required legal question remains unanswered:
What processes the patient’s symptom data into a triage output?
Without that answer, the system cannot be properly assessed for:
- transparency;
- lawful basis;
- data minimisation;
- accuracy;
- automated decision-making risk;
- clinical safety;
- equality impact;
- human oversight;
- sovereignty;
- transfer risk;
- support access;
- auditability;
- patient consent;
- or patient remedy.
That is a direct governance breach.
Patient-Access Risk
The patient-facing risk is:
symptom data submitted → undisclosed processing engine interprets symptom → urgency or pathway output generated → patient follows routing → care may be delayed, redirected, escalated, or under-prioritised
Even if a clinician-defined protocol exists, the system still executes a conversion.
The legal question is not whether clinicians helped define rules.
The legal question is:
what engine applies those rules, what data it uses, how it handles uncertainty, how it flags red-risk symptoms, and who reviews the result before access is affected?
Sovereignty Risk
The sovereignty risk is:
UK patient medical input → external SaaS system → undisclosed execution layer → possible cloud inference / logging / telemetry / analytics / support-access pathway → patient routing output
The breach does not require proof that data has already gone abroad.
The breach is the failure to disclose enough to exclude cross-border execution, modelling, analytics, telemetry, support access, or data-bleed pathways.
Core distinction:
UK storage is not UK sovereignty. UK execution, UK governance, UK model control, UK auditability, UK support boundaries, and UK legal accountability are the sovereignty questions.
Disclosure Questions
- What exact AI triage system is being deployed?
- What exact processing engine converts symptoms into outputs?
- Is the processing engine rules-based, ML-based, LLM-based, or hybrid?
- Is any third-party managed AI service used?
- Where does inference occur?
- Where does classification occur?
- Where does appointment-routing logic execute?
- Where are logs processed?
- Where is telemetry processed?
- Where is model monitoring performed?
- Where is system performance analysed?
- Is patient symptom data used to improve the model or service?
- Is patient symptom data used for behavioural-pattern analysis?
- What sub-processors are involved?
- Are any non-UK sub-processors involved?
- Can support staff outside the UK access patient requests or processing logs?
- Are backups or disaster recovery copies processed outside the UK?
- Are any EU, US, or other foreign cloud regions used?
- What transfer-risk assessment has been completed?
- What DPIA has been completed?
- What clinical safety case has been completed?
- What algorithmic transparency record has been published?
- What patient-facing transparency notice identifies AI processing?
- Can patients opt out without losing equivalent access?
- Can patients challenge a triage output?
- Can clinicians see the reasons for the triage output?
- Can clinicians override the output?
- Are overrides recorded?
- Are errors fed back into the model?
- Who is liable where the system misroutes the patient?
Evidence Relied Upon
EX-B3-01 — NHS England announcement describing AI triage within the NHS App and routing patients to appropriate NHS services.
EX-B3-02 — Public reporting describing NHS App AI triage routing patients toward GP, pharmacy, A&E, or other services.
EX-B3-03 — Rapid Health public description of Smart Triage as autonomous AI triage and booking within clinician-defined protocols.
EX-B3-04 — NHS Innovation Accelerator description of Smart Triage as fully autonomous AI-powered triage and appointment booking integrated with EMIS and TPP SystmOne.
Final Breach Position
This breach records that NHS AI triage cannot be legally assessed through storage-location statements.
The decisive issue is the execution pathway.
The public must be able to identify the system that performs the clinical-access conversion:
patient symptom → processing engine → triage output → care route
Until that is disclosed, the AI triage system remains opaque at the very point where patient access is determined.
Core line:
The breach is not where the data is kept. The breach is the undisclosed engine that makes the data act.
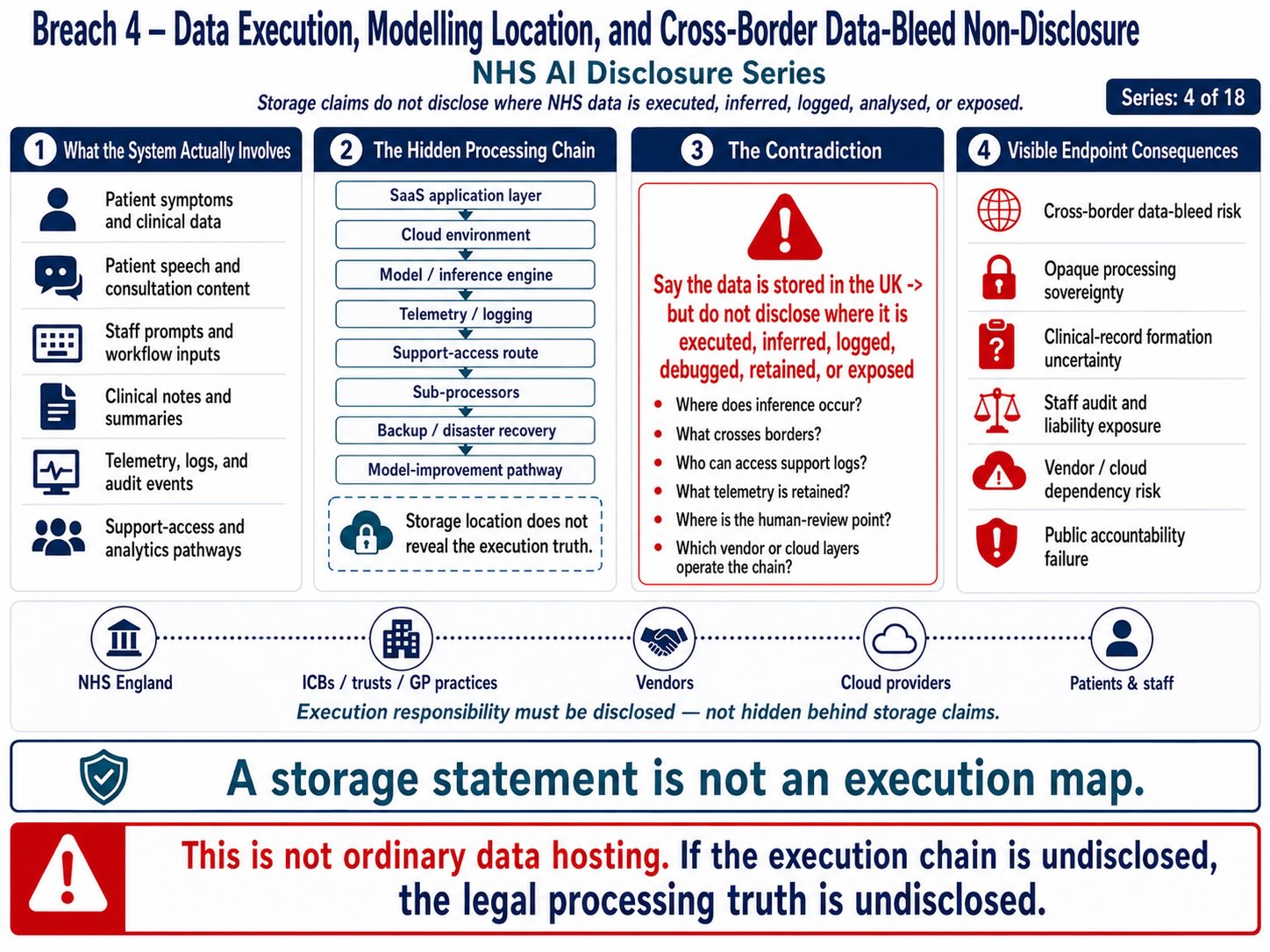
Breach 4 — Data Execution, Modelling Location, and Cross-Border Data-Bleed Non-Disclosure. This figure shows how NHS data may move beyond simple storage into execution, inference, logging, telemetry, support access, sub-processing, backup, analytics, and model-improvement pathways. The breach is the reliance on storage-location assurances before the public record discloses where data is actually executed, modelled, inferred, retained, accessed, or exposed across the processing chain.
Breach IV — Data Execution, Modelling Location, and Cross-Border Data-Bleed Non-Disclosure
Summary
This breach concerns the failure to disclose where NHS AI triage, ambient voice, Copilot-style workflow tools, patient-access systems, and staff-facing AI systems actually execute data.
The breach is not about where data is stored.
Data held on a hard drive, server, or cloud disk is passive.
The legal breach arises where patient data, staff data, symptom data, voice data, prompt data, clinical text, behavioural access data, audit trails, or metadata are:
- processed;
- executed;
- modelled;
- inferred;
- classified;
- transformed;
- summarised;
- transcribed;
- logged;
- analysed;
- monitored;
- debugged;
- used for telemetry;
- used for model improvement;
- or exposed through support-access pathways.
The disclosure position is:
storage geography does not establish processing sovereignty.
The breach mechanism is:
patient / worker input → SaaS or AI system → execution layer → model / inference / classification / transcription / summary → logs / telemetry / analytics → support / debugging / monitoring → possible cross-border data bleed
Evidence Supported
Public material concerning NHS AI triage and associated SaaS systems may describe storage on UK or England-based infrastructure. For example, a Rapid Health data-processing pack states that Rapid Health retains data on secure servers based in England on AWS infrastructure. (Practice365)
However, that does not answer where the processing engine executes the data, where inference occurs, whether logs or telemetry are generated, whether any managed AI service is used, whether support access crosses borders, or whether symptom patterns are analysed outside the storage environment.
The NHS Federated Data Platform sub-processor page separately identifies Amazon Web Services and Microsoft as sub-processors, with AWS providing cloud hosting / infrastructure and Microsoft providing AI services and associated services in UK locations. (NHS England) That confirms the broader NHS AI/data environment already relies on cloud and AI service sub-processing, not merely local storage.
The US CLOUD Act also matters to sovereignty analysis. AWS states that the CLOUD Act clarified that compelled production from service providers may include data stored inside or outside the United States. (Amazon Web Services, Inc.)
The newer US Data Security Program went into effect on 8 April 2025 under Executive Order 14117, restricting covered transactions involving bulk sensitive personal data and US government-related data with countries of concern. (Department of Justice) This is relevant because the US itself treats bulk sensitive, health, biometric, behavioural, and government-related data flows as national-security-sensitive.
Together, the evidence supports the breach question:
Where does NHS patient and workforce data act, not merely where does it rest?
Mechanism Identified
The mechanism is:
input → execution → output → exhaust
Where:
input may include patient symptoms, patient voice, clinician voice, appointment requests, documents, messages, prompts, staff activity, clinical notes, or access behaviour.
execution may include speech-to-text, triage classification, summarisation, ranking, retrieval, model inference, rules-engine processing, prompt processing, document analysis, risk scoring, or recommendation generation.
output may include triage route, urgency score, appointment booking, clinical summary, transcript, generated email, referral text, audit event, warning flag, or patient-record entry.
exhaust may include logs, telemetry, model-performance data, behavioural analytics, support tickets, error traces, security monitoring, debugging records, and improvement datasets.
The breach sits in the execution and exhaust layers.
A public statement about storage location does not answer:
- where the model runs;
- where the inference service runs;
- where speech-to-text executes;
- where triage logic executes;
- where prompt processing occurs;
- where generated summaries are produced;
- where retrieval augmented processing happens;
- where logs are processed;
- where telemetry is analysed;
- where support teams can view operational data;
- where debugging occurs;
- where backups are restored and tested;
- where model-improvement analysis occurs;
- and whether any EU, US, or other non-UK jurisdiction is involved.
Legal Frameworks Engaged
This breach engages, at minimum:
- UK GDPR Article 5(1)(a) — lawfulness, fairness, transparency.
- UK GDPR Article 5(1)(b) — purpose limitation.
- UK GDPR Article 5(1)(c) — data minimisation.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 6 — lawful basis.
- UK GDPR Article 9 — special-category health data.
- UK GDPR Article 13 — information provided to the data subject.
- UK GDPR Article 14 — information where data is generated or obtained indirectly.
- UK GDPR Article 15 — right of access.
- UK GDPR Article 16 — rectification.
- UK GDPR Article 18 — restriction of processing.
- UK GDPR Article 21 — right to object.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 28 — processor obligations.
- UK GDPR Article 30 — records of processing activities.
- UK GDPR Article 32 — security of processing.
- UK GDPR Article 35 — Data Protection Impact Assessment.
- UK GDPR Articles 44–49 — international transfer safeguards.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality.
- Caldicott Principles.
- NHS Constitution — privacy, confidentiality, informed involvement, safe care.
- Human Rights Act 1998 / ECHR Article 8 — private life, medical privacy, bodily autonomy, dignity.
- Human Rights Act 1998 / ECHR Article 14 — non-discrimination in access to rights.
- Public law rationality, proportionality and transparency.
- DCB0129 / DCB0160 clinical safety standards where execution affects clinical pathways.
- EU AI Act Article 9 — risk management.
- EU AI Act Article 10 — data governance.
- EU AI Act Article 11 — technical documentation.
- EU AI Act Article 12 — record keeping / logs.
- EU AI Act Article 13 — transparency and provision of information.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness, cybersecurity.
- EU AI Act Article 26 — deployer obligations.
- EU AI Act Article 50 — AI interaction / generated-output transparency where applicable.
- Convention 108+ — data protection safeguards.
- UNESCO Bioethics Article 9 — privacy and confidentiality.
- ICCPR Article 17 — privacy protection.
- ICESCR Article 12 — right to health.
- UN Guiding Principles on Business and Human Rights — adverse human-rights impact prevention.
Legal Duty
NHS England, ICBs, GP practices, NHS suppliers, SaaS vendors, AI vendors, cloud providers, and sub-processors must disclose the full execution chain where patient or staff data is processed.
That duty includes identifying:
- the execution location;
- the model location;
- the inference region;
- the speech-to-text processing location;
- the triage-processing location;
- the summarisation location;
- the logging location;
- the telemetry location;
- the analytics location;
- the support-access location;
- the backup and disaster-recovery processing location;
- and the model-improvement processing location.
A storage statement is not sufficient.
Where patient health data is transformed into clinical or access outputs, the controller must be able to explain the full processing path.
Breach Identified
The breach identified is the substitution of storage assurance for execution disclosure.
A public assurance that data is stored in England or the UK does not disclose:
- where the AI system runs;
- where the model executes;
- where the classification is performed;
- where the speech-to-text conversion occurs;
- where generative summarisation occurs;
- where logs are processed;
- where telemetry is inspected;
- where support engineers may access operational records;
- where cross-border legal control may arise;
- or whether patient and worker data generates behavioural patterns used outside the immediate care pathway.
This creates a data-bleed risk.
Data bleed does not require a conventional export of a database.
Data bleed may occur through:
- inference traces;
- model-performance data;
- prompt logs;
- symptom pattern analytics;
- access-behaviour data;
- error reports;
- support tickets;
- crash logs;
- security monitoring;
- audit events;
- red-flag classification data;
- correction loops;
- clinician overrides;
- and aggregated behavioural patterns.
This is why storage geography does not resolve sovereignty.
US / EU Jurisdictional Exposure
The disclosure does not assert, without proof, that NHS triage data is processed in Germany, another EU state, or the United States.
The breach is that the public record does not visibly exclude those routes.
The questions remain live because AI and SaaS systems may involve:
- UK cloud regions;
- US-controlled providers;
- EU support teams;
- EU-based monitoring or security services;
- global telemetry;
- managed AI inference;
- distributed backup;
- disaster recovery;
- analytics;
- and product-improvement processing.
The US CLOUD Act is relevant because it illustrates that location of storage alone does not resolve legal control risk for US service providers. AWS states that compelled production can include data stored outside the United States. (Amazon Web Services, Inc.)
The US Data Security Program is relevant because it demonstrates that the United States itself treats bulk sensitive personal data as a national-security matter requiring control over data transactions. (Department of Justice)
The disclosure point is therefore:
If the United States treats bulk sensitive data and behavioural data flows as strategically sensitive, NHS England cannot treat UK patient symptom, voice, access, and workflow data as ordinary SaaS exhaust.
Tribunal / Procedural Risk
This breach also has tribunal relevance because AI execution records may later become evidence.
If AI logs, prompts, summaries, access records, model outputs, audit events, or telemetry are relied upon in employment, disciplinary, regulatory, or tribunal proceedings, the affected party must know:
- where the record was created;
- by what system;
- under what processing conditions;
- whether the record is complete;
- whether the record includes generated data;
- whether timestamps are system-generated;
- whether inference outputs are recorded;
- whether logs were altered or normalised;
- whether foreign support access occurred;
- whether the AI system made assumptions;
- and whether the worker or patient can challenge the record.
Where the execution chain is undisclosed, the evidential reliability of AI-generated or AI-mediated records is unresolved.
Disclosure Questions
- Where does AI triage inference execute?
- Where does speech-to-text execute?
- Where does ambient voice summarisation execute?
- Where does Copilot prompt processing execute?
- Where does document retrieval or grounding execute?
- Where does clinical-risk classification execute?
- Where does appointment-routing logic execute?
- Where are AI logs processed?
- Where are telemetry records processed?
- Where are model-performance signals processed?
- Where are support tickets processed?
- Where are debugging records processed?
- Where are security monitoring records processed?
- Where are backups restored, tested, or processed?
- Where is disaster recovery performed?
- Are any EU/EEA jurisdictions involved?
- Are Germany, Ireland, Netherlands, France, or other EU regions used for any processing layer?
- Are any US regions used for inference, support, logging, telemetry, or model improvement?
- Are any US-controlled providers able to access data under legal compulsion?
- Are logs or telemetry treated as patient data?
- Are symptom patterns treated as health data?
- Are behavioural access patterns treated as personal data?
- Are patient or worker prompts retained?
- Are patient or worker prompts used for model improvement?
- Are clinician overrides analysed for product improvement?
- Are misroutes or corrections used as training signals?
- What transfer risk assessments have been completed?
- What UK IDTA or SCC safeguards exist where relevant?
- What sovereign exit plan exists if foreign access risk increases?
- What public document identifies the full execution chain?
Evidence Relied Upon
EX-B4-01 — Rapid Health data-processing pack stating data is retained on secure servers based in England on AWS infrastructure. (Practice365)
EX-B4-02 — NHS Federated Data Platform sub-processor page identifying Amazon Web Services and Microsoft as cloud / AI service sub-processors in UK locations. (NHS England)
EX-B4-03 — AWS CLOUD Act explanation stating compelled production can include data stored inside or outside the United States. (Amazon Web Services, Inc.)
EX-B4-04 — US Department of Justice Data Security Program page stating the programme went into effect on 8 April 2025 under Executive Order 14117. (Department of Justice)
EX-B4-05 — Rapid Health public description of Smart Triage as autonomous AI triage and booking within clinician-defined protocols. (Rapid Health)
Final Breach Position
This breach records that NHS AI sovereignty cannot be established by a storage-location statement.
The question is execution.
The public record must disclose where NHS patient and staff data is processed, modelled, inferred, classified, transformed, logged, analysed, monitored, supported, and improved.
Until that is disclosed, the system creates unresolved cross-border data-bleed risk.
Core line:
The breach is not where the data rests. The breach is where the data acts.
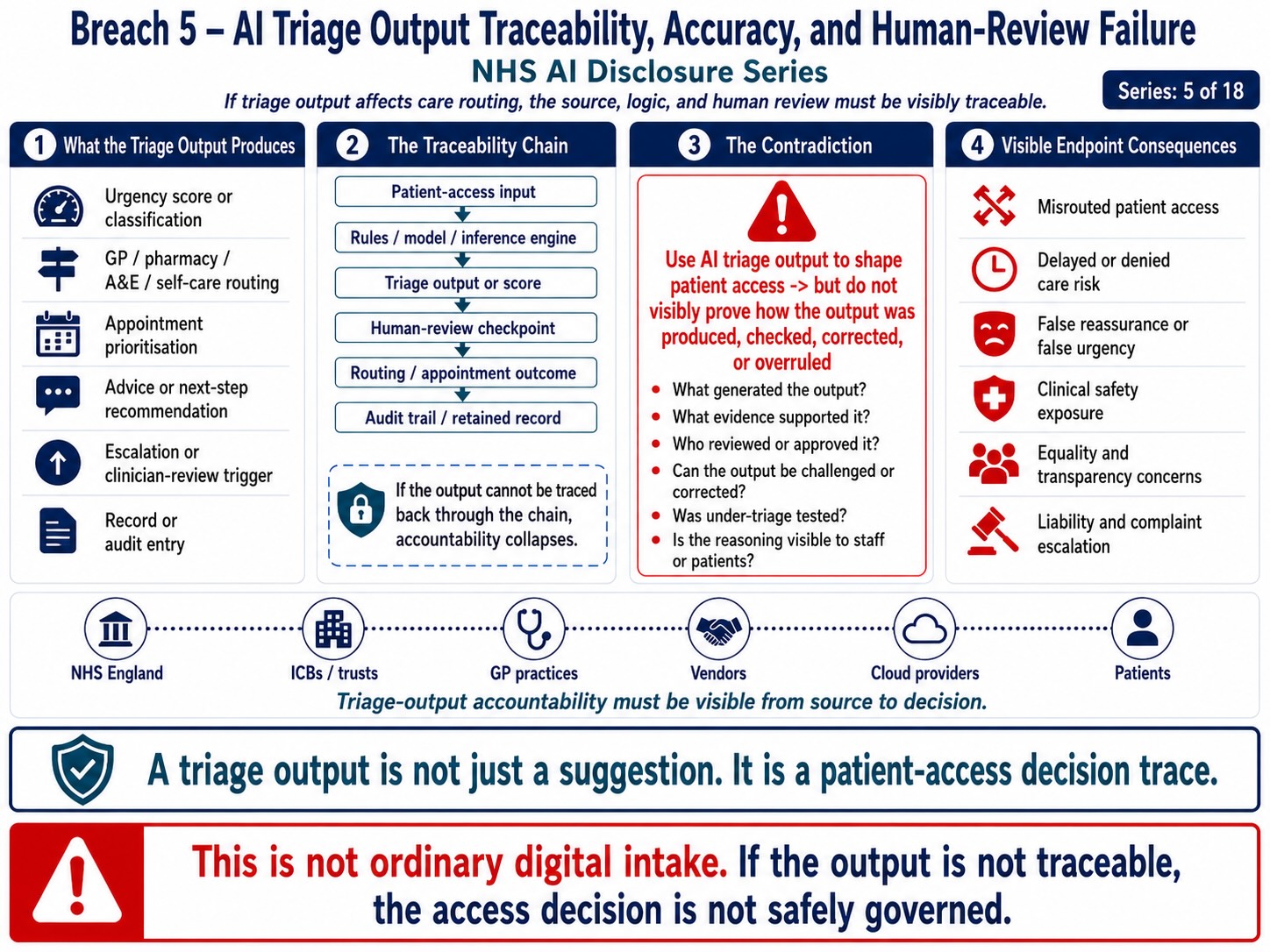
Breach 5 — AI Triage Output Traceability, Accuracy, and Human-Review Failure. This figure shows how AI triage outputs can shape patient access through urgency scoring, routing recommendations, appointment prioritisation, escalation triggers, and retained audit records. The breach is the use of triage output to influence access to care before the public record shows how the output was generated, checked, corrected, overruled, reviewed by a human, or traced from source to final decision.
Breach V — AI Triage Output Traceability, Accuracy, and Human-Review Failure
Summary
This breach concerns the point at which NHS AI triage converts patient symptom input into a healthcare-access output.
The breach is not only the existence of AI triage.
The breach is the absence of visible public proof that the output can be traced, explained, challenged, reviewed, corrected, audited, and safely relied upon before it affects patient access.
AI triage creates an output chain:
patient symptom input → adaptive questioning → AI / protocol processing → urgency classification → routing output → GP / pharmacy / A&E / community service / self-care / appointment pathway
That output may not be labelled as a diagnosis.
But it can still materially affect whether a patient reaches a clinician, how quickly they are prioritised, whether they are redirected, whether they are reassured, whether they are delayed, or whether they are escalated.
The breach mechanism is:
patient input → AI triage output → healthcare routing consequence → unclear traceability / accuracy / review / challenge route
Evidence Supported
NHS England has announced a new AI triage tool in the NHS App intended to direct patients to the most appropriate NHS service. (NHS England)
Public reporting describes the NHS App AI triage tool as recommending whether users need a GP appointment, pharmacy, A&E, or another care route, with staged rollout before national availability by April 2028. (The Guardian)
Sussex ICB states that the tool adapts questions depending on patient responses to obtain a more detailed view of the patient’s condition and directs patients to GP appointment, pharmacy, A&E, community service, or self-care advice. (Surrey Sussex ICB)
Rapid Health describes Smart Triage as autonomous AI triage and booking within clinician-defined protocols. (Rapid Health)
The NHS Innovation Accelerator describes Smart Triage as fully autonomous AI-powered triage and appointment booking for GP practices, integrated with EMIS and TPP SystmOne, and says it removes the need for manual data entry or staff intervention. (NHS Innovation Accelerator)
That evidence supports the operational pathway:
patient request → adaptive triage questions → automated / AI triage processing → route or booking output → GP clinical system / workflow integration
That is a healthcare-access classification process.
Mechanism Identified
The mechanism is:
patient describes problem → system asks questions → system interprets answers → system assigns urgency / care route → system books, redirects, prioritises, or escalates → patient follows output
The traceability issue arises because the patient, clinician, GP practice, regulator, tribunal, court, or data subject may later need to know:
- what the patient entered;
- what questions were asked;
- what answers were given;
- what symptoms were weighted;
- what red flags were considered;
- what uncertainty existed;
- what rule, model, classifier, or protocol produced the output;
- whether any alternative output was possible;
- whether a clinician reviewed the output;
- whether the patient could challenge it;
- whether the output was corrected;
- and whether the output influenced access to care.
Without that chain, the output is not safely auditable.
Legal Frameworks Engaged
This breach engages, at minimum:
- UK GDPR Article 5(1)(a) — lawfulness, fairness, transparency.
- UK GDPR Article 5(1)(b) — purpose limitation.
- UK GDPR Article 5(1)(c) — data minimisation.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 6 — lawful basis.
- UK GDPR Article 9 — special-category health data.
- UK GDPR Article 13 — information to be provided to the data subject.
- UK GDPR Article 15 — right of access.
- UK GDPR Article 16 — rectification.
- UK GDPR Article 18 — restriction of processing.
- UK GDPR Article 21 — right to object.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 30 — records of processing activities.
- UK GDPR Article 32 — security of processing.
- UK GDPR Article 35 — DPIA.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality.
- Caldicott Principles.
- NHS Constitution — informed involvement, privacy, confidentiality, safe care.
- Human Rights Act 1998 / ECHR Article 8 — medical privacy, bodily autonomy, private life.
- Human Rights Act 1998 / ECHR Article 14 — non-discrimination.
- Equality Act 2010 section 29 — services and public functions.
- Equality Act 2010 section 149 — Public Sector Equality Duty.
- Common law negligence / duty of care — foreseeable harm from misrouting, under-triage, delay, or false reassurance.
- Duty of candour where harm or near-miss arises from inaccurate triage output.
- Public law rationality and proportionality — deployment must rest on adequate evidence and safeguards.
- DCB0129 / DCB0160 clinical safety standards where clinical software affects patient pathways.
- DTAC — digital technology assessment, where applicable.
- EU AI Act Article 9 — risk management.
- EU AI Act Article 10 — data and data governance.
- EU AI Act Article 11 — technical documentation.
- EU AI Act Article 12 — record-keeping / logs.
- EU AI Act Article 13 — transparency and provision of information.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness and cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- UNESCO Bioethics Article 5 — autonomy and individual responsibility.
- UNESCO Bioethics Article 6 — consent.
- UNESCO Bioethics Article 9 — privacy and confidentiality.
- UNESCO Bioethics Article 10 — equality, justice, equity.
- ICCPR Article 17 — privacy protection.
- ICESCR Article 12 — right to health.
- UN Guiding Principles on Business and Human Rights — adverse human-rights impact prevention.
Legal Duty
NHS England, ICBs, GP practices, and AI triage vendors must ensure that patient-access outputs are transparent, accurate, auditable, clinically safe, and subject to meaningful human oversight.
That duty includes ensuring that patients and clinicians can understand:
- why a routing output was produced;
- what symptom data was used;
- what red-flag symptoms were checked;
- what uncertainty existed;
- what clinical pathway was selected;
- whether an alternative pathway was considered;
- whether a clinician reviewed the output;
- whether the patient can correct the input;
- whether the patient can challenge the output;
- whether a human can override the output;
- and whether errors are recorded and remediated.
A healthcare-access system cannot lawfully operate as an opaque output generator where the output affects care access.
Breach Identified
The breach identified is the absence of visible source-to-output accountability.
The public-facing material describes the benefit: faster access, reduced phone queues, direct booking, and routing to appropriate services.
But the legal question is:
Can the output be reconstructed?
For each triage decision, the system should be able to show:
input → questions → answers → red-flag checks → model / protocol pathway → classification → routing output → human review → final action
Without that, neither the patient nor the clinician can properly assess whether the route was safe.
That matters because AI triage may affect:
- urgency;
- care route;
- delay;
- escalation;
- self-care advice;
- access to GP;
- referral to pharmacy;
- instruction to attend A&E;
- prioritisation by practice;
- or future record context.
This is not merely administrative convenience.
It is clinical access control.
Human-Review Failure Risk
The risk is sharper where public material describes the triage as autonomous or removing the need for manual staff intervention. (NHS Innovation Accelerator)
If a system routes or books patients without manual review, the disclosure must identify:
- whether the system makes final access-routing decisions;
- whether a clinician reviews before the patient is redirected;
- whether high-risk outputs are reviewed;
- whether low-risk outputs are sampled;
- whether self-care advice is reviewed;
- whether false reassurance is monitored;
- and whether any human review occurs before harm can arise.
Human oversight cannot be decorative.
It must be placed before the system affects access or record consequence.
Patient-Access Risk
The practical risk chain is:
incomplete symptom description → adaptive questions miss context → system assigns lower urgency → patient redirected to pharmacy / self-care / delayed appointment → condition worsens before clinician review
or:
rare symptom pattern → model fails to detect red flag → system produces ordinary routing output → patient falsely reassured → delayed escalation
or:
patient misunderstands question → wrong answer entered → system routes incorrectly → error becomes pathway consequence
This risk is foreseeable because triage depends on the accuracy of patient input, question design, clinical-rule logic, symptom interpretation, and escalation thresholds.
Tribunal / Procedural Risk
This breach has procedural relevance because triage output may later become evidence in complaints, negligence claims, coronial inquiries, regulatory proceedings, employment disputes, or tribunals.
Where the output is relied upon, the affected party must be able to obtain:
- the raw patient input;
- the questions asked;
- the answers given;
- the triage pathway;
- the model or protocol version;
- the timestamp;
- the human-review record;
- the override record;
- the error-reporting record;
- and the audit trail.
If the output cannot be traced, it cannot safely be relied upon.
Disclosure Questions
- For each patient triage interaction, is the full source-to-output chain retained?
- Can the patient access the questions asked and answers given?
- Can the patient access the triage reason or pathway?
- Can a clinician see why the output was produced?
- Is the output based on rules, machine learning, LLM reasoning, or hybrid processing?
- Are red-flag symptoms explicitly checked?
- Are red-flag misses recorded?
- Is uncertainty recorded?
- Does the system generate confidence scores?
- Are confidence scores shown to clinicians?
- Are confidence scores shown to patients?
- Does the system ever route to self-care without human review?
- Does the system ever book or redirect without human review?
- Which outputs require clinician review?
- Which outputs are fully automated?
- Can patients correct mistaken symptom entries?
- Can patients challenge routing outputs?
- Can clinicians override outputs?
- Are overrides logged?
- Are overrides used to improve the model?
- Are errors fed into clinical safety review?
- Are patient complaints linked back to the triage output?
- What safety thresholds apply to under-triage?
- What safety thresholds apply to false reassurance?
- What monitoring exists for rare-condition misclassification?
- What monitoring exists for children, older adults, disabled patients, multilingual patients, and patients with communication difficulties?
- What DPIA covers the output chain?
- What clinical safety case covers the output chain?
- What equality assessment covers output reliability across patient groups?
- Who is liable where the output causes misrouting, delay, deterioration, or harm?
Evidence Relied Upon
EX-B5-01 — NHS England announcement that a new AI triage tool in the NHS App will direct patients to the most appropriate NHS service. (NHS England)
EX-B5-02 — Public reporting that the NHS App AI tool will recommend whether users need GP, pharmacy, A&E, or other care routes and is planned for national rollout by April 2028. (The Guardian)
EX-B5-03 — Sussex ICB description of adaptive questioning and routing to GP appointment, pharmacy, A&E, community service, or self-care advice. (Surrey Sussex ICB)
EX-B5-04 — Rapid Health description of Smart Triage as autonomous AI triage and booking within clinician-defined protocols. (Rapid Health)
EX-B5-05 — NHS Innovation Accelerator description of Smart Triage as fully autonomous AI-powered triage and appointment booking integrated with EMIS and TPP SystmOne, removing manual data entry or staff intervention. (NHS Innovation Accelerator)
Final Breach Position
This breach records that NHS AI triage output cannot be treated as a harmless administrative suggestion where it affects access to care.
The legally relevant point is not whether the system calls itself triage, booking, navigation, or support.
The legally relevant point is that patient symptom input becomes a healthcare-access output.
Until that output can be traced, explained, reviewed, challenged, corrected, and audited, the system remains unsafe as a national access layer.
Core line:
AI triage is not merely an app feature. It is a healthcare-access classification layer.
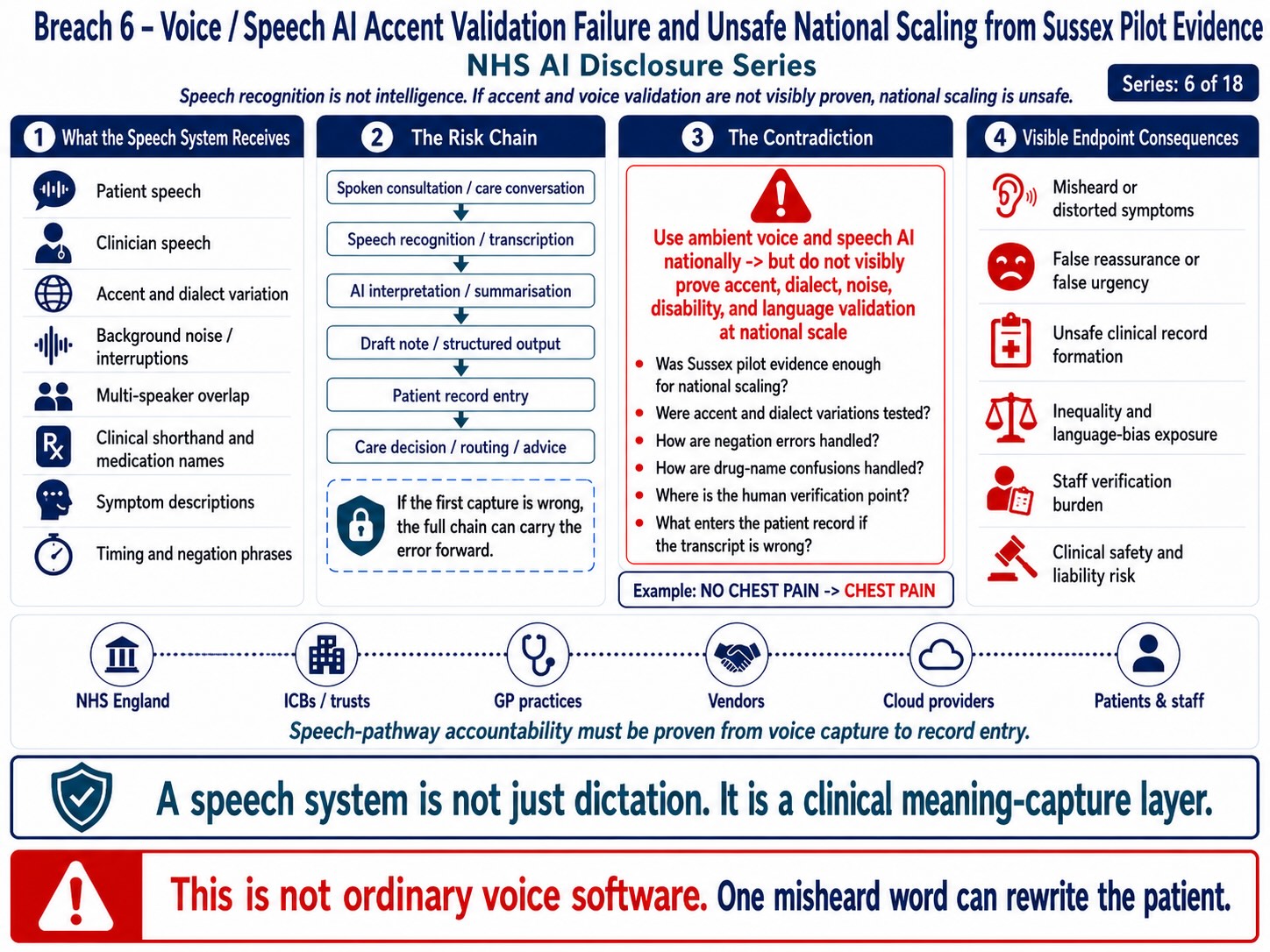
Breach 6 — Voice / Speech AI Accent Validation Failure and Unsafe National Scaling from Sussex Pilot Evidence. This figure shows how patient and clinician speech can pass through speech recognition, transcription, AI interpretation, summarisation, draft-note creation, record entry, and care-routing pathways before the accuracy of voice capture is visibly proven. The breach is the national scaling of speech-dependent AI before accent, dialect, background noise, disability, language variation, clinical shorthand, medication names, negation phrases, and human verification safeguards are transparently validated.
Breach VI — Voice / Speech AI Accent Validation Failure and Unsafe National Scaling from Sussex Pilot Evidence
Summary
This breach concerns the scaling of NHS AI triage, ambient voice technology, AI scribing, transcription, voice capture, and speech-adjacent healthcare systems from limited pilot evidence into national patient and workforce environments without visible proof of accent, dialect, language, multilingual, regional, disability, age, and clinical-noise validation.
The breach is not that a Sussex pilot occurred.
The breach is that a Sussex pilot appears to be used as national confidence evidence while the public record does not visibly show equivalent testing across the linguistic reality of the NHS.
The NHS workforce and patient population do not speak with one accent.
The NHS includes:
- Scottish accents;
- Welsh accents;
- Northern Irish accents;
- Manchester accents;
- Liverpool accents;
- Birmingham accents;
- Bradford / Yorkshire accents;
- Newcastle / North-East accents;
- London multilingual English;
- South Asian English;
- African English;
- Caribbean English;
- Eastern European English;
- speech affected by disability;
- older voices;
- anxious or distressed speech;
- and noisy clinical environments.
The breach mechanism is:
limited regional pilot → national AI rollout claim → speech / voice / triage systems deployed nationally → absent visible accent-diversity validation → foreseeable transcription, classification, routing, and record-error risk
Evidence Supported
NHS England states that the AI triage tool in the NHS App is being accelerated and that an initial trial at a GP practice in Sussex resulted in a 29% reduction in phone queues, while the tool is due to reach more than 200,000 patients within 12 months and all NHS App users by April 2028. (NHS England)
Surrey and Sussex ICB identifies the Sussex trial and states that the tool adapts questions depending on patient responses and directs patients to GP appointment, pharmacy, A&E, community service, or self-care advice. (Surrey Sussex ICB)
NHS England’s ambient scribing guidance describes AI-enabled ambient scribing products as ambient voice technologies used for clinical or patient documentation and workflow support. (NHS England)
NHS Digital states NHS England is developing a national plan to support widespread adoption of ambient scribing and AI-enabled automation. (NHS England Digital)
The speech-AI evidence base supports the risk. A 2026 study on Newcastle English found that automatic speech recognition performance remains uneven where dialect diverges from mainstream training data, with more than 3,000 transcription errors analysed and errors linked to dialect-specific phonology, local vocabulary, and social variables. (arXiv)
A 2026 UK conversational-speech AI study involving multilingual speakers from Sheffield and Bradford found bias against multilingual individuals from ethnic minority backgrounds and accent-linked misclassification risk, including South Yorkshire accent effects. (arXiv)
A healthcare speech-AI review found that datasets and research have disproportionately favoured high-resource languages, standardised accents, and narrow demographic groups, creating risk that AI speech systems may misinterpret speech from marginalised groups. (arXiv)
This evidence supports the breach question:
Has NHS AI voice, triage, transcription, and ambient scribing been validated across the actual accents, dialects, languages, and clinical speech conditions it will encounter nationally?
Mechanism Identified
The mechanism is:
patient or clinician speaks → system captures speech → speech-to-text / acoustic model processes voice → words are transcribed → AI / rules / generative model interprets text → summary, triage route, clinical note, or workflow output is generated → human or system relies on output
Accent risk enters at multiple points:
- capture risk — the system may fail to hear or segment speech correctly.
- transcription risk — accent, dialect, pronunciation, pace, stress, age, or background noise may produce wrong words.
- clinical term risk — medication names, symptom terms, body parts, dates, allergies, and dosage terms may be mistranscribed.
- triage interpretation risk — wrong words produce wrong urgency or routing.
- summary risk — AI may smooth over uncertainty into a confident note.
- record risk — the wrong summary may enter the medical record.
- liability risk — the clinician or worker may later be blamed for a system-originated voice or transcription failure.
This is not ordinary accent inconvenience.
In healthcare, accent misrecognition can alter clinical meaning.
Legal Frameworks Engaged
This breach engages, at minimum:
- UK GDPR Article 5(1)(a) — lawfulness, fairness, transparency.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 6 — lawful basis.
- UK GDPR Article 9 — special-category health data.
- UK GDPR Article 13 — patient-facing transparency.
- UK GDPR Article 15 — access to data.
- UK GDPR Article 16 — rectification of inaccurate data.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 32 — security and resilience of processing.
- UK GDPR Article 35 — DPIA.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality.
- Caldicott Principles.
- NHS Constitution — safe care, informed involvement, privacy, confidentiality, non-discriminatory access.
- Equality Act 2010 section 19 — indirect discrimination.
- Equality Act 2010 sections 20–21 — reasonable adjustments.
- Equality Act 2010 section 29 — services and public functions.
- Equality Act 2010 section 149 — Public Sector Equality Duty.
- Human Rights Act 1998 / ECHR Article 8 — medical privacy, bodily autonomy, dignity, private life.
- Human Rights Act 1998 / ECHR Article 14 — non-discrimination.
- Common law negligence / duty of care — foreseeable harm from misrecognition, misrouting, or record error.
- Duty of candour where harm or near-miss arises.
- Public law rationality and proportionality — national rollout must be evidence-based.
- DCB0129 / DCB0160 clinical safety standards where software affects patient pathways or clinical records.
- DTAC — digital technology assessment criteria where applicable.
- EU AI Act Article 9 — risk management.
- EU AI Act Article 10 — data and data governance.
- EU AI Act Article 13 — transparency and provision of information.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness, cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- UNESCO Bioethics Article 10 — equality, justice and equity.
- ICESCR Article 12 — right to health.
- UN Guiding Principles on Business and Human Rights — prevention of adverse human-rights impacts.
Legal Duty
NHS England and deploying NHS bodies must ensure that speech-dependent or speech-adjacent AI systems are validated for the population they will serve before national deployment.
That duty includes testing across:
- regional accents;
- non-native English accents;
- multilingual English;
- dialects;
- speech impairment;
- older voices;
- children’s voices where relevant;
- anxiety or distress speech;
- ward noise;
- waiting-room noise;
- telephone audio;
- mobile-device audio;
- masks or PPE muffling;
- multi-speaker consultations;
- overlapping speech;
- clinician interruption;
- and medical terminology.
A system used in healthcare must not be validated only where speech conditions are favourable or demographically narrow.
Breach Identified
The breach identified is the apparent absence of visible public proof that the AI voice, speech, triage, and ambient scribing systems have been tested across national accent and linguistic diversity before scaling.
The Sussex pilot may prove local operational benefit.
It does not prove national speech safety.
A successful local result cannot safely stand as evidence that the system works for:
- Glasgow;
- Aberdeen;
- Cardiff;
- Belfast;
- Manchester;
- Liverpool;
- Birmingham;
- Bradford;
- Sheffield;
- Newcastle;
- Leicester;
- London;
- migrant communities;
- multilingual patients;
- internationally trained NHS staff;
- or high-noise clinical settings.
This is especially important because NHS AI deployment is not only patient-facing.
It also affects staff-facing systems and ambient voice systems in which NHS workers’ voices, accents, clinical dictation, patient discussions, and verbal decisions may be processed.
Patient-Access Risk
The patient-facing risk chain is:
accent / dialect / language variation → wrong transcription or misunderstood symptom → wrong triage classification → wrong route → delayed care or false reassurance
Examples:
- “Chest tightness” being misheard or reduced to ordinary discomfort.
- Medication names being incorrectly transcribed or confused with similar-sounding drugs.
- Allergies or adverse reactions being missed, omitted, or inaccurately recorded.
- Medication dosages being misheard, misread, or incorrectly entered.
- “Numbness” being misinterpreted as pain, weakness, tingling, or another symptom.
- The location, severity, or character of pain being incorrectly transcribed.
- The timing, duration, onset, or progression of symptoms being misunderstood.
- Children’s or older patients’ speech being inaccurately processed because of age-related speech characteristics.
- Multilingual phrasing, code-switching, or non-standard English being reduced to an incorrect standard-English assumption.
The issue is not linguistic preference.
The issue is clinical safety and equality of access.
Staff-Voice Risk
The staff-facing risk is:
international NHS worker / regional NHS worker speaks → ambient voice or AI scribe mistranscribes → clinical note generated → worker expected to verify under pressure → error enters record or audit trail → worker later exposed to disciplinary or regulatory risk
This matters because NHS staff are linguistically diverse. If the system is not validated across staff accents, the employer may be creating a higher verification burden for internationally trained, regional, multilingual, or accent-diverse workers.
That engages equality, health and safety, and employment fairness.
Tribunal / Procedural Risk
This breach has tribunal relevance because voice-generated or speech-derived records may later be relied upon in:
- Disciplinary, misconduct, or capability proceedings.
- Clinical or professional negligence claims.
- Patient complaints and formal complaints investigations.
- Employment Tribunal proceedings.
- Protected disclosure and whistleblowing detriment claims.
- Professional regulatory and fitness-to-practise proceedings.
- Coronial investigations, inquests, and patient-safety investigations.
Where the record originates from speech AI, the following evidence should be disclosed:
- Whether the original audio recording remains available.
- The version of the transcript generated from the audio.
- The version of the AI-generated summary or draft note.
- The complete clinician edit history.
- Any confidence score, certainty rating, or quality indicator produced by the system.
- The full correction history, including identified errors and subsequent amendments.
- Evidence of testing across relevant accents, dialects, and speech patterns.
- Error rates broken down by accent or language group, where available.
- The device, microphone, background-noise, and environmental conditions under which the audio was captured.
- The AI model name and version used.
- The record of human review, verification, approval, or override.
- The complete audit chain showing capture, processing, transcription, summarisation, editing, correction, access, and final entry into the record.
Without that, speech-derived evidence may be procedurally unsafe.
Disclosure Questions
- Was the AI triage system tested outside Sussex before national rollout?
- Was it tested in Scotland?
- Was it tested in Wales?
- Was it tested in Northern Ireland?
- Was it tested in Manchester?
- Was it tested in Liverpool?
- Was it tested in Birmingham?
- Was it tested in Bradford?
- Was it tested in Sheffield?
- Was it tested in Newcastle?
- Was it tested in Leicester?
- Was it tested in London boroughs with high linguistic diversity?
- What accent datasets were used?
- Were non-native English speakers included?
- Were multilingual patients included?
- Were internationally trained NHS workers included?
- Were patient accents tested separately from staff accents?
- Were telephone audio conditions tested?
- Were mobile-device audio conditions tested?
- Were noisy ward and clinic settings tested?
- Were multi-speaker consultations tested?
- Were overlapping voices tested?
- Were medical terminology and medication names tested by accent group?
- Were red-flag symptom misses measured by accent group?
- Were false reassurance rates measured by accent group?
- Were under-triage rates measured by accent group?
- Were transcription error rates published by accent group?
- Were summary error rates published by accent group?
- Was an Equality Impact Assessment completed?
- Was a DPIA completed?
- Was a DCB0129 / DCB0160 clinical safety case completed?
- What error threshold was accepted before deployment?
- What mitigation exists for patients whose speech is not accurately processed?
- What equivalent non-voice route exists?
- What staff protection exists where AI mishears or mistranscribes them?
Evidence Relied Upon
EX-B6-01 — NHS England announcement that an initial Sussex GP practice trial reduced phone queues by 29% and that AI triage is being accelerated through the NHS App. (NHS England)
EX-B6-02 — Surrey and Sussex ICB report stating the tool adapts questions depending on responses and routes patients to GP appointment, pharmacy, A&E, community service, or self-care advice. (Surrey Sussex ICB)
EX-B6-03 — NHS England guidance defining AI-enabled ambient scribing / ambient voice technologies for clinical or patient documentation and workflow support. (NHS England)
EX-B6-04 — NHS Digital page stating NHS England is developing a national plan for widespread adoption of ambient scribing and AI-enabled automation. (NHS England Digital)
EX-B6-05 — 2026 Newcastle English ASR study identifying dialect-related automatic speech recognition errors and socially patterned misrecognition. (arXiv)
EX-B6-06 — 2026 UK multilingual healthcare-adjacent speech AI study finding bias against multilingual speakers and accent-linked misclassification risk. (arXiv)
EX-B6-07 — Healthcare speech AI inclusivity review identifying disproportionate reliance on high-resource languages, standardised accents, and narrow demographic groups. (arXiv)
Final Breach Position
This breach records that NHS AI voice, triage, transcription, and ambient scribing systems cannot be nationally scaled from narrow or local pilot evidence without visible accent-diversity, dialect, multilingual, disability, age, and clinical-noise validation.
A local Sussex result may support local continuation.
It cannot, without further evidence, stand as national proof that the system safely hears, interprets, transcribes, classifies, and routes the full NHS population.
Core line:
A Sussex pilot cannot stand as national accent validation for AI systems that must listen to Britain.
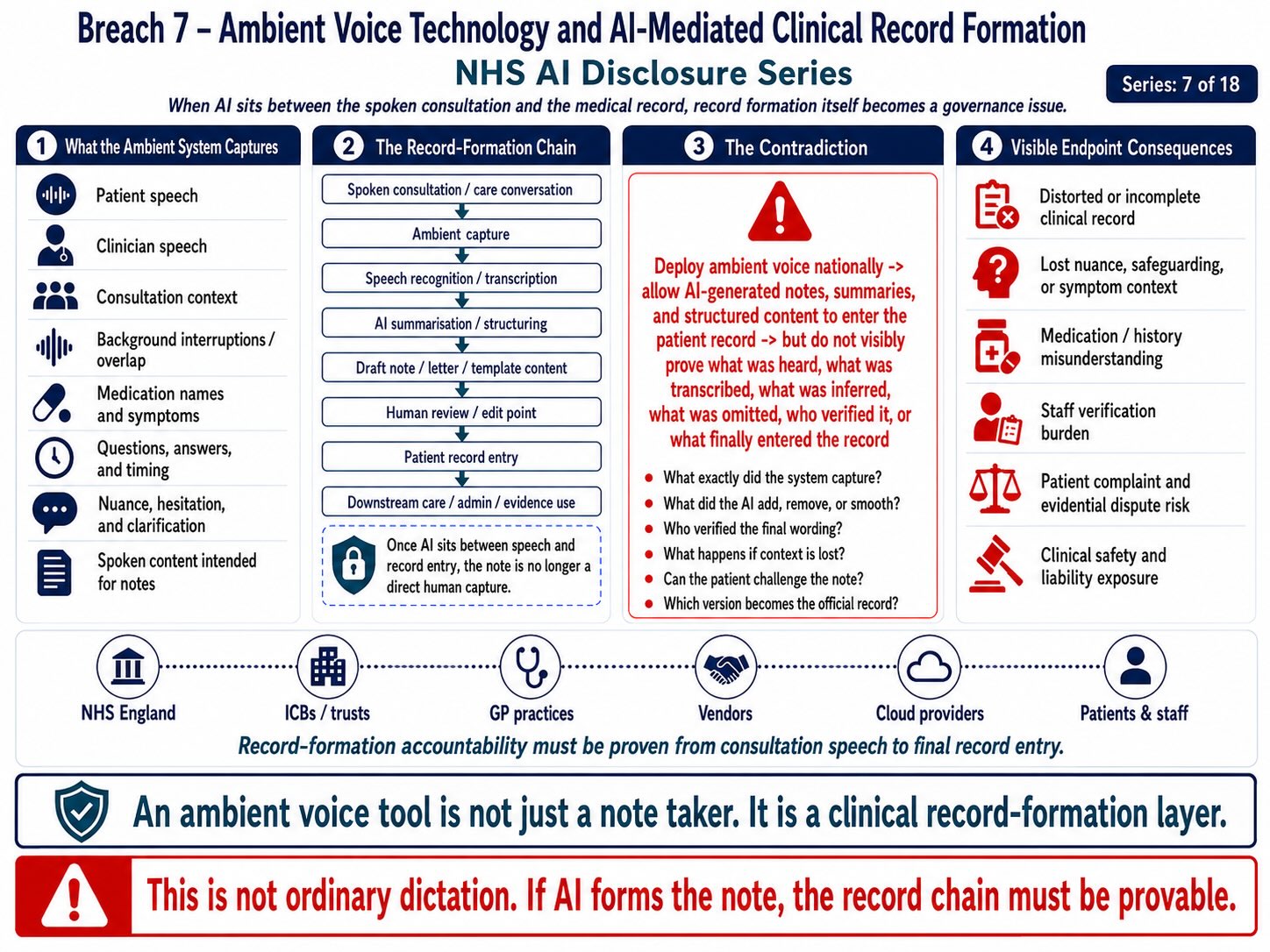
Breach 7 — Ambient Voice Technology and AI-Mediated Clinical Record Formation. This figure shows how ambient voice technology can sit between the spoken consultation and the official patient record, capturing patient speech, clinician speech, consultation context, medication names, symptoms, questions, timing, nuance, and clarification before converting them into AI-generated notes, summaries, structured content, or record entries. The breach is the formation of clinical records through an AI-mediated chain before the public record shows what was captured, transcribed, inferred, omitted, edited, verified, challenged, retained, or entered as the final medical record.
Breach VII — Ambient Voice Technology and AI-Mediated Clinical Record Formation
Summary
This breach concerns the deployment of ambient voice technology, AI scribes, AI-enabled ambient scribing products, and generative AI note-production systems into clinical and patient-documentation environments.
The breach is not that clinicians may use technology to assist note-taking.
The breach is that ambient voice systems place AI between:
the spoken clinical encounter
and
the official medical record
That creates a distinct legal risk because the patient’s spoken account, the clinician’s questions, the clinician’s explanations, the consultation context, and the resulting clinical note may pass through:
- Microphone capture of the consultation or clinical interaction.
- Speech-to-text processing of recorded audio.
- AI transcription logic used to convert speech into text.
- Generative AI summarisation of the consultation content.
- Conversion of plain language into clinical terminology, coding, or structured medical language.
- Production of a draft clinical note by the AI system.
- Clinician review, editing, verification, and approval of the draft note.
- Insertion of the final approved note into the patient’s clinical record.
- Creation and retention of audit logs documenting AI processing and user activity.
- Processing by third-party vendors, cloud providers, or other data processors.
- Collection and use of telemetry, analytics, performance monitoring, and any model training or improvement pathways.
The breach mechanism is:
patient speech → clinician speech → ambient capture → transcription → AI summarisation → draft clinical note → clinician review/edit → EPR entry → patient-record consequence
This is materially different from ordinary dictation.
Ambient voice does not merely record a clinician’s deliberate dictated note.
It captures a live consultation environment and converts conversational speech into structured clinical documentation.
Evidence Supported
NHS England guidance describes AI-enabled ambient scribing products as products featuring generative AI for use across health and care settings in England, including advanced ambient voice technologies used for clinical or patient documentation and workflow support. (NHS England)
NHS England also announced support for AI note-taking tools, stating that such tools could help doctors spend up to a quarter more time with patients. (NHS England)
Great Ormond Street Hospital’s AI-scribe FAQ states that AI scribes use ambient voice technology with generative AI to listen to conversations and generate summarised notes from patient consultations. (gosh.nhs.uk)
NHS Digital states that NHS England is developing a national plan to support widespread adoption of ambient scribing and AI-enabled automation. (NHS England Digital)
NHS Digital’s IG guidance confirms that information-governance guidance exists for AI-enabled ambient scribing products in health and care settings, including advice for patients, health and care staff, and IG professionals. (NHS England Digital)
These sources support the operational pathway:
consultation speech → ambient voice capture → generative AI processing → draft note / summary → clinician workflow → patient documentation
That is clinical-record formation through AI mediation.
Mechanism Identified
The mechanism is:
spoken consultation → captured audio → speech-to-text → AI processing → generated note → human review → record entry
The risk is that each stage can introduce error, omission, transformation, or legal ambiguity.
1. Capture layer
The system may capture patient speech, clinician speech, background voices, interruptions, emotional tone, uncertainty, family member input, or contextual details not intended as formal clinical content.
2. Transcription layer
Speech-to-text may mishear words, accents, medication names, allergies, dosages, dates, symptoms, negations, or clinical terminology.
3. Generative summarisation layer
Generative AI may condense, rephrase, reorder, infer, omit, normalise, or hallucinate content.
4. Clinical terminology layer
Conversational language may be transformed into clinical terminology, changing nuance, certainty, severity, timing, or patient meaning.
5. Human-review layer
The clinician is expected to review and correct the generated note, but this adds verification burden and creates liability if errors are missed.
6. Record-entry layer
Once entered into the EPR, the AI-mediated text becomes part of the medical record and may influence future treatment, referrals, safeguarding, diagnosis, insurance, complaints, regulation, or litigation.
That is the breach point.
Legal Frameworks Engaged
This breach engages, at minimum:
- UK GDPR Article 5(1)(a) — lawfulness, fairness, transparency.
- UK GDPR Article 5(1)(b) — purpose limitation.
- UK GDPR Article 5(1)(c) — data minimisation.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(e) — storage limitation.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 6 — lawful basis.
- UK GDPR Article 9 — special-category health data.
- UK GDPR Article 13 — patient-facing transparency where data is collected directly.
- UK GDPR Article 15 — right of access.
- UK GDPR Article 16 — rectification.
- UK GDPR Article 17 — erasure where applicable.
- UK GDPR Article 18 — restriction of processing.
- UK GDPR Article 21 — right to object.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 28 — processor obligations.
- UK GDPR Article 30 — records of processing activities.
- UK GDPR Article 32 — security of processing.
- UK GDPR Article 35 — DPIA.
- UK GDPR Articles 44–49 — international transfers where non-UK processing or access occurs.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality.
- Caldicott Principles.
- NHS Constitution — privacy, confidentiality, dignity, informed involvement, safe care.
- NHS Records Management Code of Practice.
- Professional duties of doctors, nurses, and allied health professionals regarding accurate records and confidentiality.
- Human Rights Act 1998 / ECHR Article 8 — medical privacy, bodily autonomy, dignity, private life.
- Human Rights Act 1998 / ECHR Article 14 — non-discrimination where voice / language / disability affects processing.
- Equality Act 2010 sections 19, 20–21, 29 and 149 — indirect discrimination, reasonable adjustments, services/public functions, Public Sector Equality Duty.
- Common law negligence / duty of care — foreseeable harm from inaccurate record formation.
- Duty of candour where AI-mediated record error causes harm or near-miss.
- Public law rationality and proportionality — deployment must be evidence-based and proportionate.
- DCB0129 / DCB0160 clinical safety standards where software affects clinical documentation or patient pathways.
- DTAC — digital technology assessment criteria where applicable.
- EU AI Act Article 9 — risk management.
- EU AI Act Article 10 — data and data governance.
- EU AI Act Article 11 — technical documentation.
- EU AI Act Article 12 — record keeping / logs.
- EU AI Act Article 13 — transparency and provision of information.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness and cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- EU AI Act Article 50 — AI interaction / generated-output transparency where applicable.
- UNESCO Bioethics Article 5 — autonomy and individual responsibility.
- UNESCO Bioethics Article 6 — consent.
- UNESCO Bioethics Article 9 — privacy and confidentiality.
- UNESCO Bioethics Article 10 — equality, justice and equity.
- ICCPR Article 17 — privacy protection.
- ICESCR Article 12 — right to health.
- UN Guiding Principles on Business and Human Rights — adverse human-rights impact prevention.
Legal Duty
NHS England, NHS trusts, ICBs, healthcare providers, ambient scribing vendors, AI vendors, and deploying clinicians must ensure that AI-mediated note creation is lawful, transparent, accurate, clinically safe, auditable, consented to, and subject to meaningful human control.
That duty includes:
- Informing patients that AI ambient scribing technology is being used during the consultation.
- Explaining what information is captured by the AI system.
- Explaining whether consultation audio is retained, and if so, for how long.
- Explaining whether transcripts generated from the consultation are retained.
- Explaining whether AI-generated summaries or clinical notes are retained.
- Explaining where AI processing and data storage take place.
- Explaining who supplies the AI system and who acts as the data controller and data processor.
- Explaining whether patient data is used to train, improve, evaluate, or develop AI models.
- Obtaining, recording, and maintaining an appropriate consent, objection, or opt-out pathway where applicable.
- Ensuring that patients who decline AI processing continue to receive an equivalent standard of care without disadvantage.
- Ensuring that all AI-generated notes are reviewed, verified, and approved by a clinician before being entered into the clinical record.
- Ensuring that inaccurate AI-generated information can be corrected promptly and transparensively.
- Ensuring that patients are able to access, review, and challenge inaccurate AI-generated records.
- Ensuring that applicable clinical safety standards, governance requirements, and risk controls are met.
- Ensuring that AI systems have been appropriately validated across different accents, languages, disabilities, speech patterns, and environmental noise conditions.
- Ensuring that AI-generated notes are not treated as inherently accurate or relied upon without appropriate human clinical judgement.
The legal duty attaches because the output may become the medical record.
Breach Identified
The breach identified is the creation of an AI-mediated clinical-record pathway before visible public assurance that the full capture, processing, summarisation, review, correction, retention, consent, and liability architecture has been settled.
The public benefit claim is reduced administrative burden.
The legal risk is record integrity.
An AI scribe can create a polished clinical note that appears authoritative, coherent, and complete even where the underlying conversation was uncertain, ambiguous, misheard, or partially omitted.
That creates a specific danger:
AI may convert uncertainty into apparent certainty.
This is especially important because clinical records are relied upon later by:
- The treating clinician responsible for the patient’s care.
- Other clinicians involved in the patient’s assessment, treatment, or ongoing care.
- GP practices and primary care providers.
- Hospitals, NHS trusts, and other healthcare organisations.
- Safeguarding teams and relevant safeguarding authorities.
- Insurers and indemnity providers where disclosure is lawful and necessary.
- Coroners and coronial investigators.
- Regulatory bodies and statutory oversight authorities.
- Complaints handlers and patient complaints investigators.
- Courts and judicial proceedings.
- Employment Tribunals and other tribunals with lawful authority.
- The patient, including their authorised representative where applicable.
If the AI-generated note is inaccurate, the harm can propagate.
Patient-Record Risk
The patient-record risk chain is:
spoken account → mistranscription → AI summary → clinician misses error → EPR entry → future clinician relies on wrong record → patient harm
or:
patient qualifies symptom → AI summarises as definite symptom → record overstates severity or certainty
or:
patient says “no chest pain” → transcription misses negation → note records chest pain
or:
medication / allergy / dosage mistranscribed → generated note appears clinically valid → future prescribing or treatment risk
This risk is not hypothetical in structure. It follows from the mechanism itself.
A system that converts speech into documentation must be governed at the level of clinical safety, not administrative convenience.
Consent and Consultation-Room Transparency
Ambient voice creates a consultation-room transparency issue.
The patient must know:
- Whether the consultation is being processed, monitored, or listened to by an AI system.
- Whether audio from the consultation is captured or recorded.
- Whether the audio recording is stored, and if so, for how long.
- Whether the audio recording is deleted after processing or retained.
- Whether only a transcript of the consultation is retained.
- Whether the audio, transcript, or related data is processed by a third-party vendor.
- Whether any consultation data leaves the NHS organisation for processing or storage.
- Whether consultation data is used to train, improve, evaluate, or develop AI models.
- Whether declining AI processing affects the patient’s access to care, treatment, or services.
- Whether the voices or personal information of family members, carers, interpreters, or other individuals present during the consultation are also captured, processed, or retained.
Consent cannot be buried inside a generic privacy notice where the system is actively listening to a clinical consultation.
The patient must understand the processing event at the point of care.
Clinician Liability and Verification Burden
Ambient voice also creates staff liability exposure.
The clinician may become responsible for verifying AI-generated notes under time pressure.
The verification burden includes checking:
- What information was captured from the original consultation or interaction.
- What information was not captured or omitted from the recording or transcript.
- What information was incorrectly transcribed or inaccurately recorded.
- What information was summarised or condensed by the AI system.
- What information, conclusions, or clinical observations were inferred by the AI system rather than explicitly stated.
- What information was omitted from the AI-generated output or subsequent clinical record.
- What information was translated or converted into clinical terminology, coding, or structured medical language.
- What information was ultimately entered into the patient’s clinical record, and by whom.
If the note is wrong and the clinician signs or imports it, the worker may become the visible liability endpoint for errors introduced upstream by the AI system.
This links directly to Breach I and Breach II.
Tribunal / Procedural Risk
This breach has tribunal and procedural relevance because AI-generated clinical notes may later be relied upon in:
- Clinical negligence claims.
- Disciplinary, capability, or misconduct proceedings.
- Employment Tribunal proceedings.
- Disability discrimination and reasonable adjustment claims.
- Protected disclosure and whistleblowing detriment claims.
- Safeguarding disputes and investigations.
- Patient complaints and formal complaints procedures.
- Professional regulatory and fitness-to-practise proceedings.
- Coronial investigations and inquests.
- Data protection complaints and regulatory investigations.
Where an AI-generated note is relied upon, the following records should be disclosed:
- The status and availability of the original audio recording.
- The transcript generated from the audio recording.
- The original AI-generated draft note.
- The final clinician-reviewed and edited clinical note.
- The complete edit history showing all amendments.
- The AI model name and version used to generate the note.
- The prompt, input, or generation process used to produce the output, where available.
- Any confidence score, certainty rating, or quality indicator produced by the AI system.
- The correction history showing identified errors and subsequent amendments.
- Vendor processing details, including any third-party processing or cloud services.
- The applicable retention policy for audio, transcripts, prompts, outputs, and related records.
- The patient’s consent record, including any refusal or withdrawal of consent.
- The complete audit log recording creation, access, modification, review, and use of the AI-generated note.
Without that evidence chain, the AI-mediated record may be procedurally unsafe.
Disclosure Questions
- Which ambient voice / AI scribing systems are being deployed?
- Which NHS organisations are deploying them?
- Which vendors are involved?
- Is audio captured?
- Is audio retained?
- How long is audio retained?
- Is transcript text retained?
- Is the AI-generated draft retained?
- Is the final clinician-edited version retained?
- Is edit history retained?
- Are patients told at the point of consultation?
- Can patients refuse?
- Is equivalent care provided if they refuse?
- Are family members or carers captured?
- Are interpreters captured?
- Where does speech-to-text processing occur?
- Where does generative summarisation occur?
- What model or vendor performs summarisation?
- Are transcripts or summaries used for model improvement?
- Are logs or telemetry generated?
- Are confidence scores produced?
- Are confidence scores visible to clinicians?
- Are hallucinations or omissions monitored?
- Are medication names, allergies, dosages, dates, and negations specifically tested?
- Are accent, dialect, language, disability, and noise error rates published?
- What clinical safety case has been completed?
- What DPIA has been completed?
- What equality impact assessment has been completed?
- What records management policy applies?
- Who is liable where an AI-mediated note is wrong?
Evidence Relied Upon
EX-B7-01 — NHS England guidance describing AI-enabled ambient scribing products, including ambient voice technologies used for clinical or patient documentation and workflow support. (NHS England)
EX-B7-02 — NHS England announcement backing AI note-taking tools to increase face-to-face care time. (NHS England)
EX-B7-03 — Great Ormond Street Hospital FAQ stating that AI scribes use ambient voice technology with generative AI to listen to conversations and generate summarised consultation notes. (gosh.nhs.uk)
EX-B7-04 — NHS Digital page stating NHS England is developing a national plan for widespread adoption of ambient scribing and AI-enabled automation. (NHS England Digital)
EX-B7-05 — NHS Digital IG guidance page for AI-enabled ambient scribing products in health and care settings. (NHS England Digital)
EX-B7-06 — Reuters legal analysis identifying legal risks from ambient scribes, including errors or hallucinations, consent, privacy, malpractice liability, and regulatory compliance. (Reuters)
EX-B7-07 — 2026 medical speech-to-text research noting that clinical speech systems must handle specialist terminology, contextual ambiguity, measurements, abbreviations, and clinical shorthand precisely in safety-critical settings. (arXiv)
EX-B7-08 — 2026 ambient AI note research showing clinician editing transforms AI draft notes into final clinical documentation and varies by clinician, confirming that draft-to-final record formation is an active transformation process. (arXiv)
Final Breach Position
This breach records that ambient voice technology is not merely note-taking support.
It is an AI-mediated record-formation system.
It captures speech, transforms it into text, generates clinical summaries, requires clinician verification, and may enter the official medical record.
Until the capture, processing, consent, transcription, summarisation, correction, retention, audit, and liability pathway is disclosed, the system creates unresolved risk to patient confidentiality, record accuracy, clinical safety, and worker accountability.
Core line:
Ambient voice places AI between the spoken clinical encounter and the official medical record.
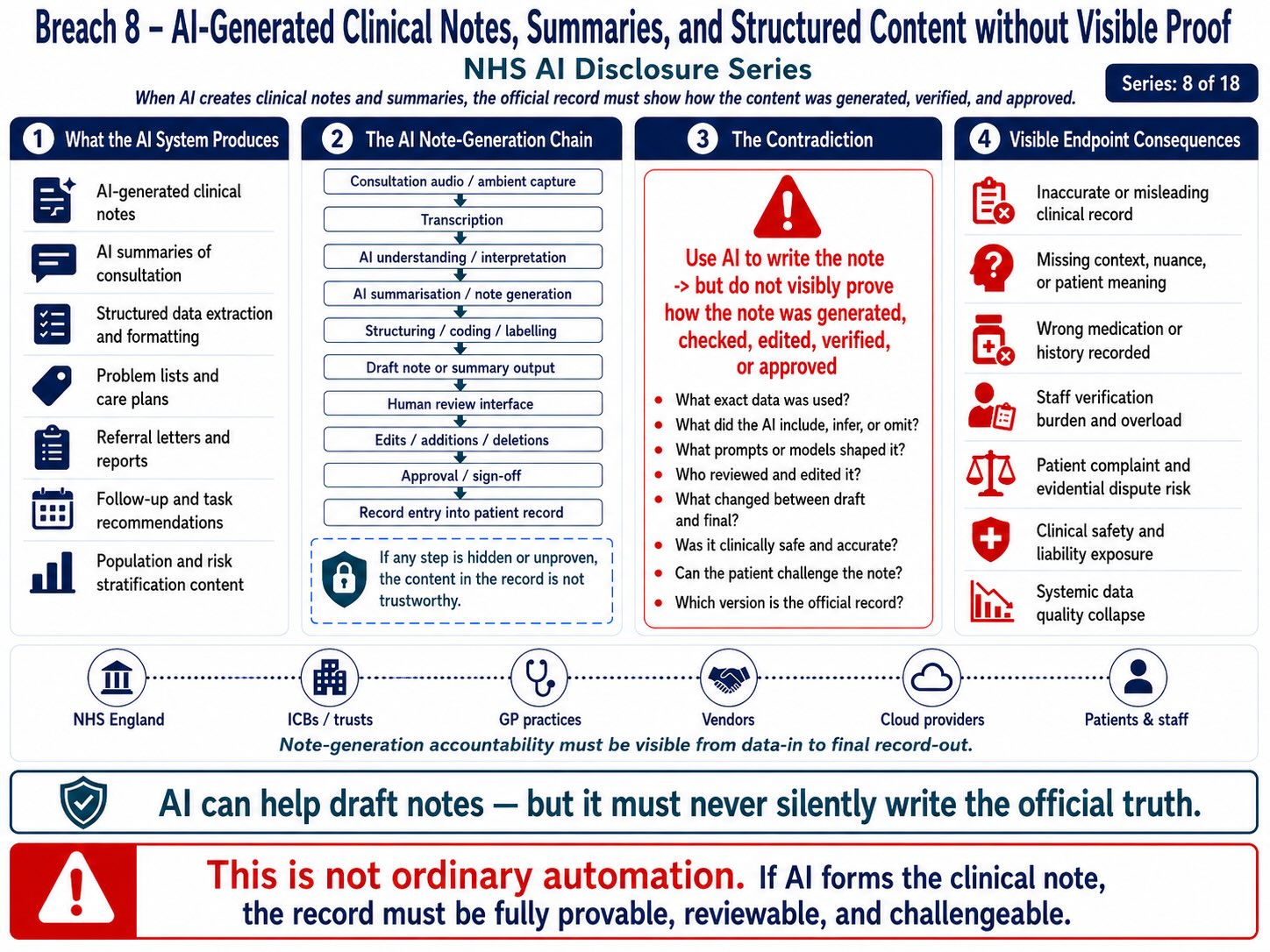
Breach 8 — AI-Generated Clinical Notes, Summaries, and Structured Content without Visible Proof. This figure shows how AI-generated clinical notes, summaries, structured data, problem lists, care plans, referral letters, follow-up tasks, and risk-stratification content can enter the patient record through a note-generation chain involving transcription, interpretation, summarisation, coding, human review, editing, approval, and record entry. The breach is the creation of official clinical content before the public record shows what data was used, what the AI included or omitted, who checked or edited it, which version became official, whether the patient can challenge it, and whether the final record is clinically safe, reviewable, and provable.
Breach VIII — Patient Consent, Transparency, and Meaningful Choice Failure
Summary
This breach concerns the absence of visibly settled patient-facing consent, transparency, objection, opt-out, and equivalent-access safeguards where NHS AI systems are deployed into patient access, triage, ambient voice, clinical documentation, and SaaS-mediated processing environments.
The breach is not simply that AI is being used.
The breach is that patients may be exposed to AI-mediated healthcare access or AI-mediated record formation without being clearly told:
- That AI is being used as part of the patient’s care or administrative process.
- What AI system or technology is being used.
- What categories of personal, clinical, or patient data are being processed.
- What the AI system does and the purpose for which it is used.
- Whether the AI affects patient access, triage, routing, clinical summarisation, documentation, prioritisation, or decision support.
- Where the data is processed, stored, or otherwise executed.
- Who supplies the AI system, and who acts as the data processor or service provider.
- Whether voice recordings, transcripts, symptom data, or other clinical inputs are retained.
- Whether audit logs, metadata, telemetry, or other processing records are generated and retained.
- Whether patient data or AI interactions are used to train, improve, evaluate, or develop AI models.
- Whether patients are able to refuse or opt out of AI processing.
- Whether refusing AI processing preserves an equivalent standard of access to care, treatment, and clinical services without disadvantage.
The breach mechanism is:
patient seeks NHS care → AI triage / ambient voice / AI documentation introduced → patient data processed → output affects access or record → patient consent / transparency / refusal / equivalent-access route unclear
Evidence Supported
NHS England states that the NHS App AI triage tool will direct patients to the most appropriate NHS service. Public reporting describes this as recommending whether patients need a GP appointment, pharmacy, A&E, or another route, with staged rollout before national availability by April 2028. (The Guardian)
NHS England’s ambient scribing guidance describes AI-enabled ambient scribing products as generative-AI products used across health and care settings, including ambient voice technologies used for clinical or patient documentation and workflow support. (NHS England)
NHS Digital information-governance guidance states that ambient scribes may assist health and care professionals by producing summaries following consultations, and that the guidance covers IG considerations for organisations adopting ambient scribes for individual care purposes. (NHS England Digital)
NHS England’s ambient-scribing publication states that guidance exists for NHS technology leaders implementing ambient scribing products in health and care settings. (NHS England)
External legal commentary on NHS ambient scribes states that patients must be informed at the start of each interaction if an ambient scribe is in use and given a clear chance to object. (Mills & Reeve)
That evidence supports the operational concern:
AI is being inserted into patient-facing care pathways, but the consent and transparency architecture must be explicit at the point of interaction, not buried in general digital policy.
Mechanism Identified
The mechanism differs across AI routes.
AI triage mechanism
patient enters symptoms → system asks adaptive questions → AI / automated processing produces route → patient is directed toward GP / pharmacy / A&E / self-care / appointment pathway
Consent question:
Did the patient understand that an AI or automated system was processing their symptom disclosure into a healthcare access output?
Ambient voice mechanism
patient speaks in consultation → ambient system captures speech → speech-to-text / generative AI produces note → clinician reviews → note may enter record
Consent question:
Did the patient understand that the clinical conversation was being captured and processed by an AI system, and could they object without detriment to care?
Staff-assisted AI mechanism
staff uses AI tool on patient-related workflow → patient data or patient-adjacent text enters AI workflow → output supports correspondence, documentation, prioritisation, or administration
Consent question:
Was the patient told that AI may process their information beyond ordinary human administration?
The consent breach occurs because each route involves a different patient-facing risk, but public assurances often flatten them into “technology” or “digital support.”
Legal Frameworks Engaged
This breach engages, at minimum:
- UK GDPR Article 5(1)(a) — lawfulness, fairness, transparency.
- UK GDPR Article 5(1)(b) — purpose limitation.
- UK GDPR Article 5(1)(c) — data minimisation.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(e) — storage limitation.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 6 — lawful basis.
- UK GDPR Article 9 — special-category health data.
- UK GDPR Article 13 — information to be provided where personal data is collected from the data subject.
- UK GDPR Article 14 — information where personal data is obtained or generated indirectly.
- UK GDPR Article 15 — right of access.
- UK GDPR Article 16 — rectification.
- UK GDPR Article 17 — erasure where applicable.
- UK GDPR Article 18 — restriction of processing.
- UK GDPR Article 21 — right to object.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 28 — processor obligations.
- UK GDPR Article 30 — records of processing activities.
- UK GDPR Article 32 — security of processing.
- UK GDPR Article 35 — DPIA.
- UK GDPR Articles 44–49 — international transfers where non-UK processing or access occurs.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality.
- Caldicott Principles.
- NHS Constitution — privacy, confidentiality, dignity, informed involvement, safe care.
- Human Rights Act 1998 / ECHR Article 8 — medical privacy, bodily autonomy, dignity and private life.
- Human Rights Act 1998 / ECHR Article 14 — non-discrimination.
- Equality Act 2010 sections 19, 20–21, 29 and 149 — indirect discrimination, reasonable adjustments, services/public functions, Public Sector Equality Duty.
- Common law negligence / duty of care — foreseeable harm from misrouting, misdocumentation, or uninformed AI processing.
- Public law fairness, rationality and proportionality.
- DCB0129 / DCB0160 clinical safety standards where AI affects clinical pathways or records.
- EU AI Act Article 13 — transparency and provision of information.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness and cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- EU AI Act Article 50 — transparency for AI interaction and AI-generated output where applicable.
- UNESCO Bioethics Article 5 — autonomy and individual responsibility.
- UNESCO Bioethics Article 6 — consent.
- UNESCO Bioethics Article 9 — privacy and confidentiality.
- UNESCO Bioethics Article 10 — equality, justice and equity.
- ICCPR Article 17 — privacy protection.
- ICESCR Article 12 — right to health.
- UN Guiding Principles on Business and Human Rights — prevention of adverse human-rights impacts.
Legal Duty
NHS England, ICBs, GP practices, NHS trusts, vendors, processors, and deploying clinicians must ensure that patients receive clear, timely, understandable, and route-specific information where AI is used in their care pathway.
That duty includes explaining:
- Whether AI is being used as part of the patient’s care or administrative process.
- Whether use of the AI system is mandatory, optional, or capable of being declined.
- What the AI system is designed to do and the purpose for which it is used.
- Whether the AI system influences patient access, triage, clinical documentation, decision support, or administrative workflow.
- What categories of patient, personal, or confidential data are processed by the AI system.
- Whether patient or clinician voice recordings are captured.
- Whether audio recordings are retained, and if so, for how long.
- Whether transcripts generated from voice recordings are retained.
- Whether AI-generated summaries, notes, or clinical documentation are retained.
- Whether symptom data, assessment responses, or clinical inputs are retained.
- Whether audit logs, metadata, telemetry, or other processing records are created and retained.
- Whether patient data or AI interactions are used to train, improve, evaluate, or develop the AI system or related products.
- Who is the data controller responsible for the processing.
- Who acts as the data processor.
- Who supplies, develops, or operates the AI system as the vendor.
- Where AI processing and data storage take place.
- Whether patient data is transferred or processed outside the United Kingdom or other applicable jurisdiction.
- How patients may object to or opt out of AI processing where such a right exists.
- How patients can request the correction of inaccurate AI-generated information or records.
- Whether an equivalent standard of care, access, and treatment remains available without the use of AI.
Transparency must occur at the point where the patient is affected.
A general privacy notice is not enough where AI is actively mediating access, listening to a consultation, or creating a clinical record.
Breach Identified
The breach identified is the apparent absence of a visibly settled, patient-facing AI consent and meaningful-choice architecture across NHS AI triage and ambient voice deployment.
There are three separate consent failures.
1. Triage consent failure
A patient may enter symptoms into an NHS App or GP access route believing they are using a digital form, while the system actually converts their data into an automated triage or routing output.
That requires clear AI-specific transparency.
2. Ambient voice consent failure
A patient may speak during a consultation without fully appreciating that an AI system is capturing, transcribing, processing, summarising, and potentially contributing to the medical record.
That requires point-of-care notice and a clear opportunity to object.
3. Equivalent access failure
If refusal of AI triage or ambient voice creates delay, worse access, extra burden, or reduced service quality, then the consent is not meaningful.
A choice is not meaningful if declining AI means poorer access to care.
Patient Autonomy Risk
The patient autonomy risk is:
patient needs care → AI route presented as normal NHS route → patient complies to obtain access → patient data processed → patient has no real understanding or practical alternative
That is not meaningful consent.
In healthcare, consent must not be reduced to interface compliance.
Clicking through an app, continuing a consultation, or failing to object to a notice does not necessarily show informed agreement to AI-mediated processing, model execution, voice capture, vendor processing, or data-retention consequences.
Clinical and Record Risk
Consent is linked to clinical safety because the patient may behave differently if they know AI is involved.
A patient may:
- Speak less openly or candidly during consultations.
- Decline to disclose sensitive symptoms or personal information.
- Avoid discussing mental health, sexual health, or other highly sensitive matters.
- Withhold information relating to domestic abuse, safeguarding, coercion, or exploitation.
- Avoid disclosing information they believe could affect their immigration status, employment, or benefits.
- Feel concerned about conversations being recorded, retained, or analysed by AI systems.
- Misunderstand who will receive, access, or process their personal information.
- Incorrectly assume that AI-generated outputs have been reviewed, verified, or approved by a human clinician before being relied upon or entered into the clinical record.
That affects the quality of care.
Tribunal / Procedural Risk
This breach has tribunal and procedural relevance because consent records, AI notices, opt-out records, patient objections, and generated outputs may later be relied upon in:
- Clinical negligence claims.
- Data protection complaints and regulatory investigations.
- Employment disputes and Employment Tribunal proceedings.
- Whistleblowing and protected disclosure detriment claims.
- Equality Act 2010 discrimination and reasonable adjustment claims.
- Disciplinary, capability, or misconduct proceedings.
- Professional regulatory and fitness-to-practise proceedings.
- Coronial investigations and inquests.
- Judicial review proceedings.
Where AI consent or refusal is disputed, the evidential record should demonstrate:
- What information the patient was provided about the AI system or process.
- When that information was provided.
- How the information was communicated.
- What the patient expressly consented to or refused.
- Whether the patient’s refusal affected access to treatment, services, or care.
- Whether a reasonable non-AI or alternative pathway was available.
- Whether any AI-generated output, recommendation, summary, or record was incorporated into the patient’s clinical record.
Without that chain, reliance on the AI-derived record or pathway may be procedurally unsafe.
Disclosure Questions
- Are patients explicitly told when AI triage is used?
- Are patients explicitly told when ambient voice or AI scribing is used?
- Are patients told the name of the AI system or vendor?
- Are patients told whether AI affects access, routing, booking, prioritisation, or documentation?
- Are patients told whether their data is processed by a third-party SaaS provider?
- Are patients told where execution and inference occur?
- Are patients told whether audio is captured?
- Are patients told whether audio is retained?
- Are patients told whether transcripts are retained?
- Are patients told whether AI-generated summaries are retained?
- Are patients told whether symptom data is used for model improvement?
- Are patients told whether logs or telemetry are created?
- Are patients told whether data may cross borders?
- Can patients refuse AI triage?
- Can patients refuse ambient voice?
- Can patients refuse AI processing without losing equivalent access?
- What non-digital route exists?
- What non-AI route exists?
- Is refusal recorded?
- Is consent recorded?
- Is objection recorded?
- Can patients later withdraw consent or object?
- Can patients access the AI-generated output?
- Can patients correct inaccurate AI-generated content?
- Can patients challenge a triage route?
- Can patients challenge an AI-generated note?
- What happens where the patient lacks capacity?
- What happens where a family member, carer, interpreter, or child is captured?
- What happens where domestic abuse, mental health, sexual health, immigration, employment, or safeguarding disclosures are made?
- Who is liable where consent was unclear?
Evidence Relied Upon
EX-B8-01 — NHS App AI triage public reporting describing recommendation/routing to GP, pharmacy, A&E, or other care routes. (The Guardian)
EX-B8-02 — NHS England guidance describing AI-enabled ambient scribing products featuring generative AI and ambient voice technologies for clinical or patient documentation and workflow support. (NHS England)
EX-B8-03 — NHS Digital IG guidance for AI-enabled ambient scribing products, describing use for producing consultation summaries and IG considerations for individual care. (NHS England Digital)
EX-B8-04 — NHS England publication page for ambient scribing guidance for technology leaders implementing products in health and care settings. (NHS England)
EX-B8-05 — External legal commentary stating patients should be informed at the start of each interaction if an ambient scribe is in use and given a clear chance to object. (Mills & Reeve)
EX-B8-06 — Academic analysis of health-data opt-out and consent framing in England, identifying concern that defaults and framing can weaken meaningful choice in health-data processing. (arXiv)
EX-B8-07 — Healthcare AI agency framework proposing informing, assessment, and consent as core principles for patient agency in AI-enabled healthcare. (arXiv)
Final Breach Position
This breach records that NHS AI deployment cannot lawfully proceed as if patient acceptance is automatic merely because the system is presented through the NHS App, GP access route, or clinical consultation.
Where AI mediates access, captures voice, generates notes, processes symptoms, or creates outputs capable of entering the care pathway, the patient must be clearly informed and given a meaningful route to object or use an equivalent non-AI pathway.
Core line:
Consent is not meaningful if the patient must accept AI to access care.
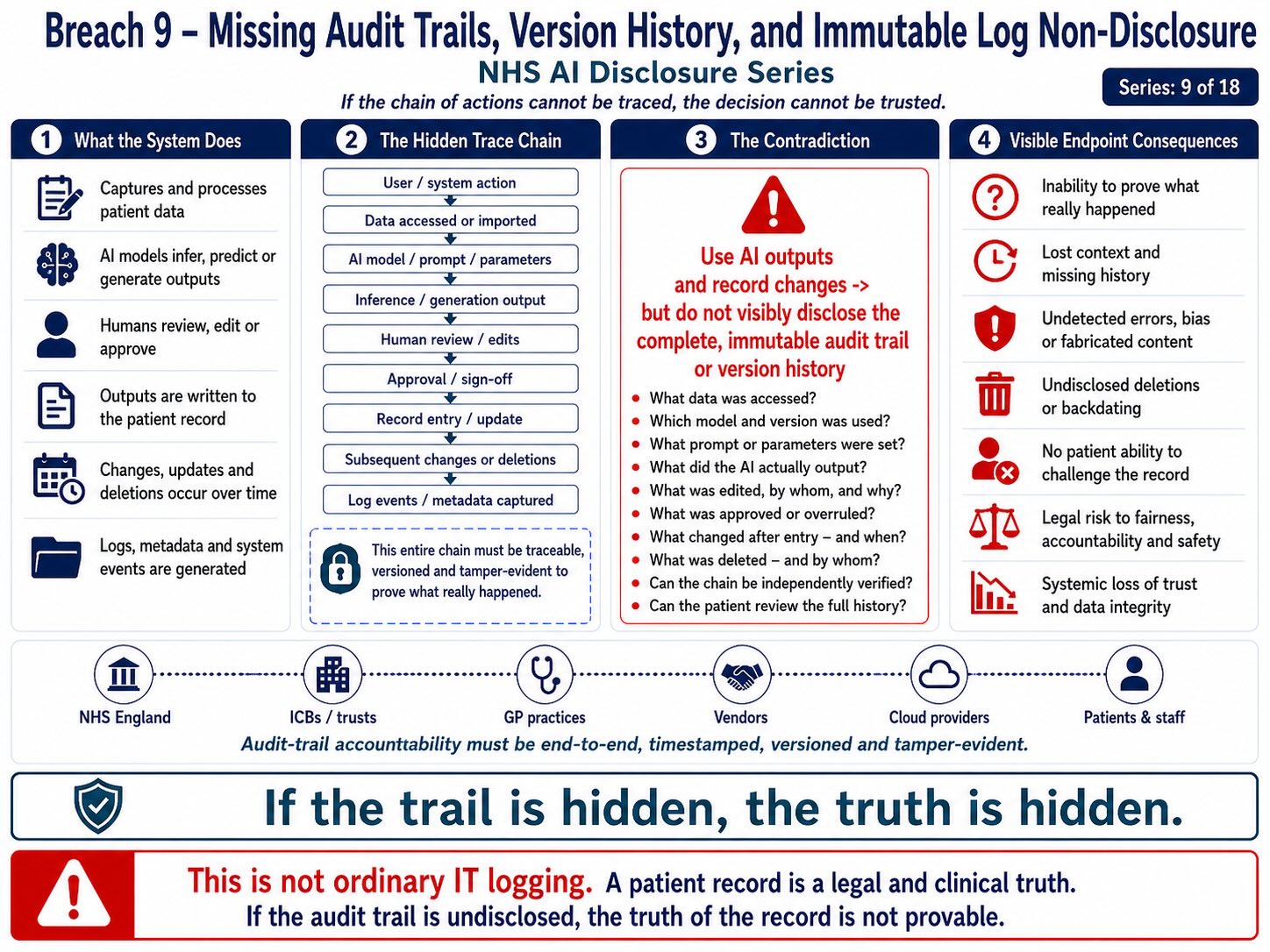
Breach 9 — Pseudonymisation, Re-Identification, and Pattern-Correlation Failure. This figure shows how pseudonymised NHS data can still create re-identification risk when patient records, demographic details, access patterns, clinical context, location signals, timestamps, quasi-identifiers, and external datasets are correlated through AI or analytics systems. The breach is the treatment of pseudonymisation as if it were anonymity before the public record proves that pattern-correlation, linkage attack, inference, and re-identification safeguards have been tested, governed, and disclosed.
Breach IX — Pseudonymisation, Re-Identification, and Pattern-Correlation Failure
Summary
This breach concerns the risk that NHS AI systems treat pseudonymisation, de-identification, anonymisation, or name-removal as sufficient protection where AI systems can still process, correlate, infer, reconstruct, or expose identity through patterns.
The breach is not limited to whether a patient’s name, NHS number, address, or date of birth is visible.
The breach is that identity in AI systems is not confined to direct identifiers.
Identity may also exist through:
- Symptom sequences and patterns of clinical presentation.
- Appointment timing, frequency, and attendance history.
- Diagnosis clusters and combinations of clinical conditions.
- Medication histories and prescribing patterns.
- Rare diseases, uncommon conditions, or low-prevalence diagnoses.
- Postcode districts and geographic location indicators.
- Age bands or demographic groupings.
- Ethnicity indicators or demographic markers.
- GP practice identifiers and registered healthcare providers.
- Hospital episodes, admissions, and treatment records.
- Referral pathways and patterns of care progression.
- Voice characteristics and biometric voice patterns.
- Accent profiles and speech-recognition characteristics.
- Consultation behaviour and patterns of clinical interaction.
- User access behaviour and system usage patterns.
- Triage responses and assessment outcomes.
- Clinician override decisions and intervention patterns.
- AI model telemetry and operational monitoring data.
- System logs, audit trails, and processing records.
- AI prompts, inputs, and user interactions.
- Metadata associated with users, records, devices, or AI processing.
The breach mechanism is:
patient data stripped of obvious identifiers → AI / SaaS / analytics system processes quasi-identifiers and behavioural patterns → pattern correlation reconstructs or narrows identity → patient remains identifiable in substance
Core distinction:
Name removal is not identity removal.
Evidence Supported
The ICO’s anonymisation guidance states that anonymisation turns personal data into anonymous information so it falls outside data protection law, but the entire premise of the guidance is that this requires careful assessment of identifiability and risk, not merely removal of a name. (ICO)
NHS England’s own information-governance guidance states that pseudonymised data remains personal data and cannot be shared freely. (NHS England)
NHS England’s FDP privacy notice says personal data will only be processed where strictly necessary and that access should be restricted to de-identified or anonymous data where users do not need to know identity. (NHS England)
NHS England’s FDP information-governance material states that de-identified data may be used by analysts to produce dashboards and that only the minimum necessary de-identified data should be used for the specific purpose. (NHS England)
Academic healthcare anonymisation literature also identifies that quasi-identifiers and sensitive attributes create re-identification risk, and that healthcare anonymisation must evaluate quasi-identifier dimensions rather than simply remove direct identifiers. (arXiv)
That evidence supports the breach position:
pseudonymisation is not a final answer where AI systems process pattern-rich healthcare data at scale.
Mechanism Identified
The mechanism is:
direct identifiers removed → quasi-identifiers remain → AI system processes patterns → cross-reference or inference narrows identity → patient becomes re-identifiable or functionally identifiable
In AI-mediated NHS systems, the relevant data may include:
- Patient-reported symptom inputs.
- Triage questions, answers, and assessment responses.
- Appointment history and attendance records.
- Referral pathways and onward-care routes.
- Clinical summaries and generated patient overviews.
- Medication names, prescriptions, and treatment references.
- Allergy and adverse-reaction information.
- Clinician notes, observations, and recorded assessments.
- Text generated from patient or clinician voice recordings.
- Ambient voice transcripts and background clinical conversations.
- Patient-access logs and system activity records.
- Device identifiers, technical data, and usage information.
- Dates, times, and event timestamps.
- GP practice codes and organisational identifiers.
- Local care-pathway markers and service-location indicators.
- AI model telemetry, processing records, and performance data.
Each item may appear harmless in isolation.
Combined, they can create a recognisable identity pattern.
The risk increases where data is processed across systems:
NHS App → AI triage → GP system → ambient voice → EPR → analytics → logs → vendor support → cloud telemetry
At that point, identity can be inferred through system behaviour even when explicit identifiers are suppressed.
Legal Frameworks Engaged
This breach engages, at minimum:
- UK GDPR Article 5(1)(a) — lawfulness, fairness, transparency.
- UK GDPR Article 5(1)(b) — purpose limitation.
- UK GDPR Article 5(1)(c) — data minimisation.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(e) — storage limitation.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 6 — lawful basis.
- UK GDPR Article 9 — special-category health data.
- UK GDPR Article 13 — information to be provided to data subjects.
- UK GDPR Article 14 — information where data is not obtained directly.
- UK GDPR Article 15 — right of access.
- UK GDPR Article 16 — rectification.
- UK GDPR Article 17 — erasure where applicable.
- UK GDPR Article 18 — restriction of processing.
- UK GDPR Article 21 — right to object.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 28 — processor obligations.
- UK GDPR Article 30 — records of processing activities.
- UK GDPR Article 32 — security of processing.
- UK GDPR Article 35 — DPIA.
- UK GDPR Articles 44–49 — international transfer safeguards where pattern data or telemetry crosses borders.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality.
- Caldicott Principles.
- NHS Constitution — privacy, confidentiality, informed involvement, safe care.
- Human Rights Act 1998 / ECHR Article 8 — medical privacy, private life, bodily autonomy, dignity.
- Human Rights Act 1998 / ECHR Article 14 — non-discrimination where pattern correlation affects protected groups.
- Equality Act 2010 sections 19, 29 and 149 — indirect discrimination, services/public functions, Public Sector Equality Duty.
- Public law rationality and proportionality — pseudonymisation claims must be evidence-based.
- EU AI Act Article 9 — risk management.
- EU AI Act Article 10 — data and data governance.
- EU AI Act Article 11 — technical documentation.
- EU AI Act Article 12 — record keeping / logs.
- EU AI Act Article 13 — transparency and provision of information.
- EU AI Act Article 15 — accuracy, robustness and cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- Convention 108+ — special-category data safeguards.
- UNESCO Bioethics Article 9 — privacy and confidentiality.
- ICCPR Article 17 — privacy protection.
- UDHR Article 12 — privacy, honour and reputation.
- OECD Privacy Guidelines — collection limitation, purpose specification, use limitation, security safeguards.
- UN Guiding Principles on Business and Human Rights — adverse human-rights impact prevention.
Legal Duty
NHS England, NHS bodies, AI vendors, SaaS vendors, cloud providers, processors, and sub-processors must ensure that pseudonymisation, anonymisation, de-identification, or masking is not treated as legally sufficient unless re-identification risk has been assessed in the actual processing environment.
That duty requires assessment of:
- Direct identifiers.
- Indirect identifiers.
- Quasi-identifiers.
- Metadata associated with records, users, or systems.
- Behavioural patterns capable of identifying individuals.
- Clinical rarity and uncommon medical characteristics.
- Small-cohort re-identification risk.
- Geographic narrowing through location-based information.
- Temporal narrowing through dates, times, or event sequences.
- Voice identity and biometric voice characteristics.
- Accent, speech, and linguistic pattern recognition.
- Symptom sequences capable of identifying an individual.
- Referral pathways and patterns of clinical progression.
- User access behaviour and system interaction patterns.
- AI model telemetry and operational monitoring data.
- System logs, audit trails, and processing records.
- AI prompts, inputs, and user interactions.
- AI-generated outputs and derived inferences.
- Cross-system correlation capable of enabling re-identification.
The duty is not satisfied by saying “names are removed.”
The duty is satisfied only where the controller can show that re-identification is not reasonably likely in context.
Breach Identified
The breach identified is the apparent reliance on de-identification or pseudonymisation language without visible public proof that AI-era pattern correlation has been assessed.
AI systems increase re-identification risk because they are designed to detect structure in large datasets.
A human may not recognise a patient from a medication pattern, appointment rhythm, postcode district, and rare condition.
An AI system may.
The breach is therefore:
traditional pseudonymisation claim → AI pattern-processing environment → quasi-identifiers remain → re-identification / functional-identification risk not visibly answered
This breach applies across:
- AI-powered triage systems.
- Ambient voice technology for clinical documentation.
- AI-assisted clinical scribing systems.
- Copilot-style summarisation and drafting tools.
- Federated Data Platform (FDP) analytics and decision-support systems.
- Patient access, authentication, and activity logs.
- Workforce monitoring, audit trails, and activity records.
- AI model telemetry, performance monitoring, and operational logging.
- Cloud-based and Software-as-a-Service (SaaS) AI processing environments.
Patient-Identity Risk
The patient-identity risk chain is:
patient name removed → symptom sequence remains → appointment time remains → GP location remains → rare condition remains → medication remains → demographic marker remains → AI correlation narrows identity
or:
voice/audio removed → transcript remains → accent markers remain → idiom remains → clinical detail remains → location and pathway remain → identity can be inferred
or:
direct identifier removed → telemetry records behaviour → same pattern appears across systems → patient becomes linkable
This is why identity must be treated as pattern, not label.
Sovereignty and Data-Bleed Risk
This breach connects directly to Breach IV.
Even if the primary database remains in the UK, pattern data may bleed through:
· logs;
· telemetry;
· analytics;
· model monitoring;
· support tickets;
· security events;
· error reports;
· summary outputs;
· prompt traces;
· and product-improvement signals.
That means re-identification risk cannot be assessed only at the database level.
It must be assessed at the execution, exhaust, analytics, and support layers.
Tribunal / Procedural Risk
This breach also has procedural relevance because pseudonymised or AI-generated data may be relied upon in proceedings.
If a party relies on de-identified, aggregated, pseudonymised, or AI-derived data in:
- Employment Tribunal proceedings.
- Protected disclosure and whistleblowing claims.
- Data protection complaints and regulatory investigations.
- Clinical negligence and professional negligence claims.
- Judicial review proceedings.
- Regulatory, professional, or disciplinary proceedings.
- Coronial investigations and inquests.
- Clinical complaints, patient safety investigations, and healthcare complaints procedures.
the affected party must be able to test:
- Whether the data was genuinely anonymous or merely pseudonymised.
- Whether the cohort or dataset was sufficiently small to increase the risk of identification.
- Whether the data could reasonably be linked back to an identifiable individual.
- Whether AI processing created new identifiers, inferred attributes, or re-identification risks.
- Whether the AI-generated output was derived from, or revealed information about, personal data.
- Whether logs, prompts, metadata, or processing records were retained and could be associated with an individual.
- Whether the data or AI-generated output could prejudice, disadvantage, or adversely affect an identifiable patient or worker.
Without that, the evidence may be procedurally unsafe.
Disclosure Questions
- Has re-identification risk been assessed for AI triage data?
- Has re-identification risk been assessed for ambient voice transcripts?
- Has re-identification risk been assessed for AI-generated clinical summaries?
- Has re-identification risk been assessed for Copilot prompts and outputs?
- Has re-identification risk been assessed for audit logs?
- Has re-identification risk been assessed for telemetry?
- Has re-identification risk been assessed for support tickets?
- Has re-identification risk been assessed for model-performance data?
- Are quasi-identifiers catalogued?
- Are symptom sequences treated as potential identifiers?
- Are rare conditions treated as potential identifiers?
- Are appointment rhythms treated as potential identifiers?
- Are voice or accent patterns treated as potential identifiers?
- Are GP practice or postcode-area markers treated as potential identifiers?
- Are medication combinations treated as potential identifiers?
- Are clinician override patterns treated as potential identifiers?
- Are behavioural access patterns treated as personal data?
- Are prompts treated as personal data?
- Are generated summaries treated as personal data?
- Are logs and telemetry treated as personal data?
- Are pseudonymised datasets processed by AI models?
- Are de-identified datasets used for model improvement?
- Can vendor staff access pseudonymised pattern data?
- Can sub-processors access de-identified but linkable data?
- What threshold is used to determine “anonymous”?
- What small-cohort controls exist?
- What linkage-attack testing has been performed?
- What model-inversion or membership-inference testing has been performed?
- What DPIA addresses AI-era re-identification risk?
- What public document explains the re-identification analysis?
Evidence Relied Upon
EX-B9-01 — ICO anonymisation guidance explaining anonymisation as the process of turning personal data into anonymous information, requiring assessment of identifiability. (ICO)
EX-B9-02 — NHS England IG guidance stating pseudonymised data remains personal data and cannot be shared freely. (NHS England)
EX-B9-03 — NHS FDP privacy notice stating personal data is processed only where strictly necessary and that access is restricted to de-identified or anonymous data where identity is not needed. (NHS England)
EX-B9-04 — NHS FDP categories-of-personal-data page stating de-identified data may be used by analysts to produce dashboards, with data minimisation and controlled access. (NHS England)
EX-B9-05 — Healthcare anonymisation research identifying quasi-identifiers and sensitive attributes as central to healthcare re-identification risk. (arXiv)
EX-B9-06 — Healthcare anonymisation review explaining that anonymisation alone may not be sufficient and identifying reconstruction / re-identification attack risks. (arXiv)
Final Breach Position
This breach records that NHS AI systems cannot rely on pseudonymisation, de-identification, or name-removal as if those measures automatically resolve medical-data sovereignty.
In AI systems, identity may arise from correlation, behaviour, clinical pattern, voice, timing, geography, metadata, and system exhaust.
The legal question is not simply whether the name is visible.
The legal question is whether the person remains inferable.
Core line:
In AI systems, the pattern is the person.
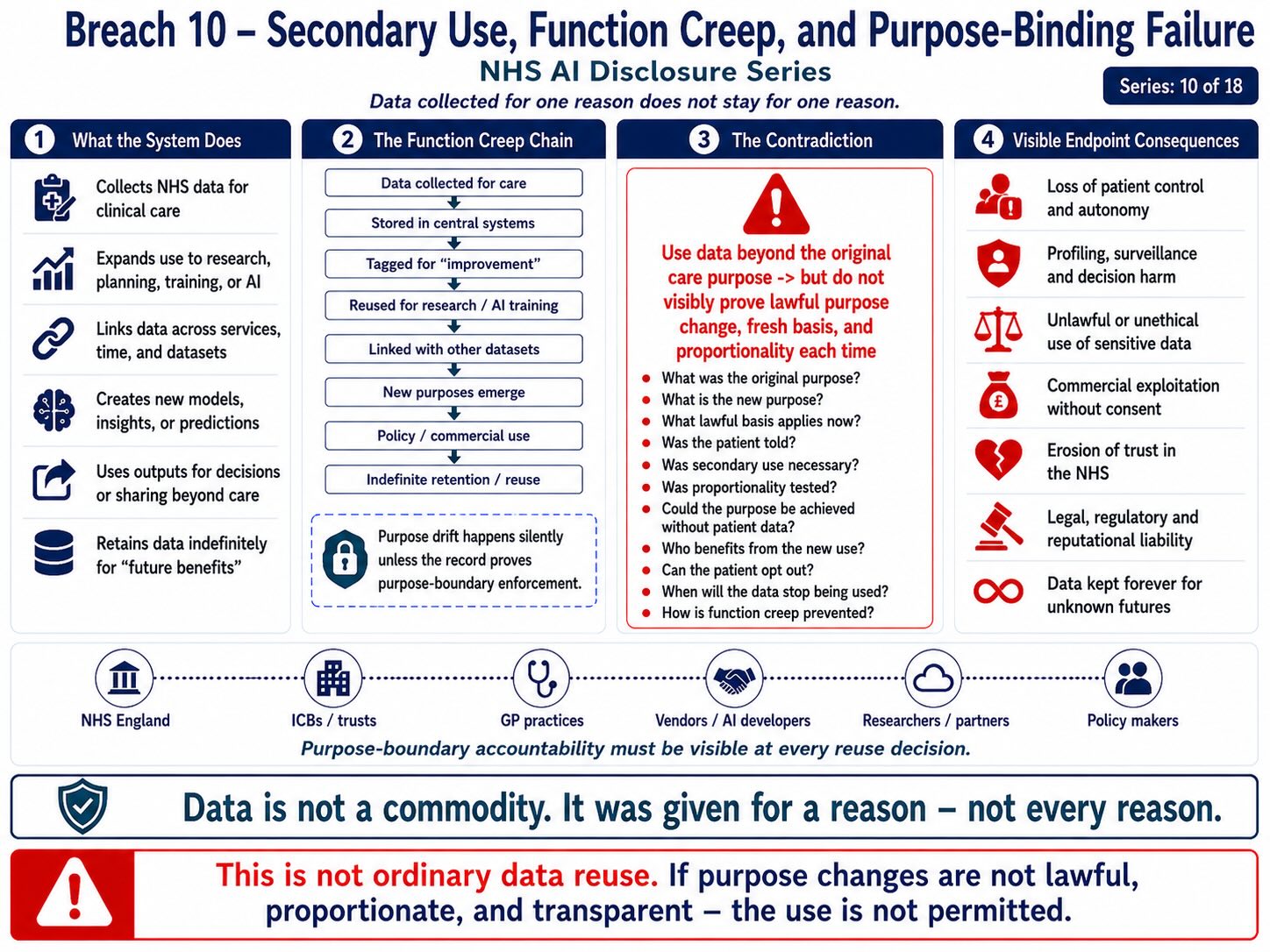
Breach 10 — Staff Digital Competence, Training, and Professionalisation Mismatch. This figure shows how NHS staff may be placed inside AI-mediated triage, workflow, documentation, audit, and patient-record systems before training, competence, role boundaries, professional accountability, escalation routes, and verification duties are visibly proven. The breach is the deployment of AI tools into staff workflows before the public record shows that workers have been properly trained, assessed, protected, and professionally supported to understand, challenge, verify, or safely refuse AI-generated outputs.
Breach X — Staff Digital Competence, Training, and Professionalisation Mismatch
Summary
This breach concerns the mismatch between the scale and speed of NHS AI deployment and the visible settlement of staff competence, AI literacy, training, professional standards, role boundaries, and liability protection.
The breach is not that NHS staff cannot learn AI systems.
The breach is that staff may be placed into AI-mediated working environments before the employer has visibly established:
- Role-specific AI training appropriate to the worker’s duties and responsibilities.
- Clear permissible-use boundaries defining authorised use of AI systems.
- Clear prohibited-use boundaries identifying unacceptable or restricted AI use.
- Patient-data input rules governing what information may and may not be entered into AI systems.
- Prompt safety rules to minimise the risk of inaccurate, unsafe, or inappropriate AI outputs.
- Duties to verify, review, and validate AI-generated outputs before reliance or use.
- Procedures for identifying, reporting, and correcting AI hallucinations, errors, or unsafe outputs.
- The purpose, retention, access, and potential consequences of AI audit logs.
- Boundaries governing the use of AI-related records for disciplinary, regulatory, or performance management purposes.
- Equality-adjusted training and reasonable adjustments for workers with protected characteristics.
- Alignment between AI use, professional accountability, and applicable regulatory, statutory, and professional standards.
The breach mechanism is:
mass AI deployment → mixed staff competence → patient-adjacent use → AI output / audit trail / error risk → worker verification burden → possible disciplinary or tribunal consequence
Core line:
You cannot professionalise after exposure and threaten before competence.
Evidence Supported
NHS England announced rollout of Microsoft 365 Copilot to more than 500,000 NHS staff after a trial involving more than 30,000 workers across 90 NHS organisations, with the claim that AI-powered administrative support could save an average of 43 minutes per staff member per day. (NHS England)
NHS England’s digital workforce material states that professional membership and registration are being introduced for the NHS digital, data and technology workforce, bringing DDaT closer to other established NHS professions and supporting safe delivery of digital services underpinning patient care. (NHS England Workforce)
BCS reported that NHS England expects digital staff to enrol on a professional membership programme developed with FEDIP, describing this as recognition of the public accountability, ethical practice, and competence needed in digital health. (BCS)
NHS England’s Digital Academy states its mission is to empower all NHS staff to develop the digital skills needed to enable healthcare services. (NHS England Workforce)
NHS England also issued public warning language that staff may face dismissal or prison for inappropriate patient-record access. (NHS England)
Those facts create the competence contradiction:
digital health is being professionalised because it requires competence and public accountability, yet AI tools are being pushed to hundreds of thousands of staff whose roles may not be digital-specialist roles.
Mechanism Identified
The mechanism is:
staff member receives AI tool → uses AI in patient-adjacent work → AI retrieves / drafts / summarises / classifies / rewrites / analyses → staff expected to verify → audit trail is created → error or misuse may later be attributed to the worker
This creates a competence gap where ordinary NHS workers may be expected to understand:
- Prompt engineering risks, including inaccurate, incomplete, or misleading inputs.
- AI hallucination risks resulting in false, fabricated, or misleading outputs.
- Limits on the entry of patient, personal, or confidential data into AI systems.
- Confidentiality boundaries governing the use and disclosure of sensitive information.
- Retrieval risks arising from inaccurate, incomplete, or contextually inappropriate information retrieval.
- The reliability, accuracy, and limitations of AI-generated outputs.
- Audit log creation, retention, access, and governance requirements.
- Vendor processing arrangements, including third-party access to data and AI services.
- Model limitations, including known performance constraints and operational boundaries.
- Algorithmic bias and the risk of discriminatory or unequal outcomes.
- Errors arising from automated summarisation, transcription, or content generation.
- Potential disciplinary, regulatory, or legal consequences arising from AI use or misuse.
A mass productivity rollout cannot assume that all staff possess AI-governance competence.
Legal Frameworks Engaged
This breach engages, at minimum:
- Health and Safety at Work etc. Act 1974 section 2 — employer duty to provide a safe system of work.
- Management of Health and Safety at Work Regulations 1999 — risk assessment.
- HSE workplace stress management standards — workload, control, support, role clarity, change management.
- Employment Rights Act 1996 section 98 — fairness in dismissal.
- Employment Rights Act 1996 section 47B — protected-disclosure detriment.
- Employment Rights Act 1996 section 103A — automatic unfair dismissal for protected disclosure.
- Public Interest Disclosure Act 1998.
- ACAS Code of Practice on Disciplinary and Grievance Procedures.
- Common law implied duty of mutual trust and confidence.
- Employer common law duty of care.
- Equality Act 2010 sections 19, 20–21 and 39 — indirect discrimination, reasonable adjustments, employment protections.
- Equality Act 2010 section 149 — Public Sector Equality Duty.
- Human Rights Act 1998 / ECHR Article 8 — dignity, reputation, private life, psychological integrity.
- Human Rights Act 1998 / ECHR Article 6 — fair process where AI-use records are relied upon.
- Natural justice — right to know and answer the case.
- Employment Tribunal Rules / overriding objective — fair and just handling of AI-related evidence.
- UK GDPR Article 5(1)(a) — fairness and transparency in processing staff and patient data.
- UK GDPR Article 5(1)(d) — accuracy of AI-generated / audit data.
- UK GDPR Article 13 — information to staff where data is collected from them.
- UK GDPR Article 15 — access to staff data and AI-use records.
- UK GDPR Article 16 — rectification of inaccurate staff data.
- UK GDPR Article 22 — automated decision-making / profiling where AI-derived records affect staff.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 35 — DPIA for high-risk processing.
- Common Law Duty of Confidentiality where patient data is involved.
- Caldicott Principles.
- NHS Constitution — safe care, confidentiality, dignity and staff standards.
- EU AI Act Article 13 — transparency and provision of information.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness and cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- UN Guiding Principles on Business and Human Rights — avoid adverse human-rights impacts through organisational systems.
Legal Duty
NHS England and deploying NHS bodies must provide a safe, fair, role-specific, equality-adjusted competence framework before exposing staff to AI systems whose use may affect patient data, clinical documentation, workflow outputs, audit trails, disciplinary decisions, or tribunal evidence.
That duty includes ensuring staff understand:
- What AI tools they are authorised to use.
- What categories of patient or confidential data must not be entered into AI systems.
- Whether AI-generated outputs may be relied upon for clinical, administrative, or operational decisions.
- How AI-generated outputs should be verified before use.
- What AI hallucinations are and how they may arise in practice.
- What steps to take when AI-generated output is incorrect, misleading, or unsafe.
- How corrections to AI-generated output should be recorded and documented.
- Whether prompts, inputs, and AI-generated outputs are logged and retained.
- Whether AI logs identify individual workers or users.
- Whether AI logs may be used for performance management, disciplinary action, or regulatory investigation.
- How workers can challenge inaccurate or misleading AI usage records.
- How unsafe AI use should be reported or escalated.
- How whistleblowing protections apply where staff raise concerns about AI safety, governance, or compliance.
Training must precede liability.
Breach Identified
The breach identified is the apparent mismatch between:
mass deployment of AI tools to hundreds of thousands of staff
and
visible competence, training, professionalisation, and liability protection architecture.
Digital health staff are being moved toward professional registration because digital systems underpin patient care and require public accountability, ethical practice, and competence. (NHS England Workforce)
That logic does not disappear when AI is placed in the hands of non-specialist users.
If anything, it becomes more important.
AI tools can produce outputs that look polished, confident, and complete, while still being incomplete, inaccurate, hallucinated, unsafe, or outside policy.
The staff member is then placed in the position of verifier, editor, risk assessor, data-governance checker, and potential liability endpoint.
That is the breach.
Workforce and Stress Risk
The competence gap creates stress risk because staff may face:
- Pressure to use AI to meet productivity, performance, or efficiency targets.
- Uncertainty about what use of AI was permitted, prohibited, or expected.
- Fear of making errors involving patient data or confidential information.
- Fear of disciplinary action arising from AI-related mistakes or misuse.
- Fear of AI-generated audit logs being used for performance management or disciplinary purposes.
- Lack of confidence in the accuracy, reliability, or safety of AI-generated outputs.
- Increased verification burden resulting from the need to review, check, and validate AI outputs.
- Difficulty identifying, correcting, or challenging AI-generated errors or system decisions.
- Exposure to public criminal-threat messaging associated with AI misuse or governance failures.
Where staff are expected to adopt AI while also being warned of severe consequences for record misuse, the employer must assess occupational stress and role clarity.
The public threat language cannot sit on top of an unresolved competence architecture.
Equality Risk
The competence breach may fall unevenly across staff groups.
Risk may be higher for:
· staff with lower digital literacy;
· older staff;
· disabled staff;
· neurodivergent staff;
· staff with language barriers;
· internationally trained staff;
· lower-band administrative staff;
· agency staff;
· bank staff;
· part-time staff;
· staff with limited training time;
· staff under workload pressure.
That engages the Equality Act and Public Sector Equality Duty because the same AI tool may not impose the same burden on every worker.
Tribunal / Procedural Risk
This breach has direct tribunal relevance because staff AI use may later become evidence in employment disputes.
- Whether staff were adequately trained before the alleged misuse occurred.
- Whether the employer’s AI policies, guidance, and procedures were clear, accessible, and consistently applied.
- Whether AI-generated logs, audit trails, and system records were complete, accurate, and reliable.
- Whether AI retrieval or outputs were initiated by the user or automatically generated by the system.
- Whether the worker had a reasonable opportunity to understand, verify, and appropriately use the AI tool.
- Whether workload, time pressure, or operational demands affected the worker’s ability to use the AI system safely and correctly.
- Whether disability, language, literacy, or other protected characteristics affected the worker’s competence or interaction with the AI system.
- Whether the employer made reasonable adjustments to accommodate any disability or protected characteristic affecting AI use.
- Whether protected disclosures concerning AI safety, governance, or compliance resulted in detriment to the worker.
- Whether any disciplinary action or dismissal was procedurally fair in light of the evidence, training, system design, and surrounding circumstances.
Potential tribunal issues include:
A tribunal cannot fairly assess AI-related misconduct unless the competence and training chain is disclosed.
Disclosure Questions
- What AI training was delivered before Copilot licence activation?
- Was training mandatory?
- Was training role-specific?
- Was training assessed or merely offered?
- Were staff tested for AI literacy before use?
- Were staff told what patient data they may input?
- Were staff told what patient data they must not input?
- Were staff told whether prompts are logged?
- Were staff told whether outputs are retained?
- Were staff told whether logs may be used in discipline?
- Were staff told how to challenge inaccurate AI logs?
- Were staff told how to identify hallucinations?
- Were staff trained on verification duties?
- Were staff trained on data-execution risk, not just data storage?
- Were staff trained on vendor / cloud / processor boundaries?
- Were staff trained on AI-generated clinical documentation risk?
- Were staff trained on triage-output risk?
- Were staff trained on patient consent and refusal pathways?
- Were equality-adjusted training routes provided?
- Were reasonable adjustments provided for disabled staff?
- Were agency, bank, part-time, lower-band, and non-clinical staff included?
- Was occupational stress risk assessed?
- Was workload impact assessed?
- Was the ACAS disciplinary route updated for AI-related allegations?
- Was a tribunal disclosure protocol created for AI logs and outputs?
- Were staff told how PIDA protections apply if they report AI safety concerns?
- What professional standards apply to non-DDaT staff using AI?
- Who signs off competence before AI use in patient-adjacent work?
- Who is liable where training was absent or insufficient?
- What evidence proves training preceded exposure?
Evidence Relied Upon
EX-B10-01 — NHS England announcement that more than 500,000 staff will receive Microsoft 365 Copilot access after a 30,000-worker trial across 90 NHS organisations. (NHS England)
EX-B10-02 — NHS England digital workforce material stating professional membership and registration are being introduced for the DDaT workforce to support safe delivery of digital services underpinning patient care. (NHS England Workforce)
EX-B10-03 — BCS report stating NHS England expects digital staff to enrol in a professional registration programme developed with FEDIP, recognising public accountability, ethical practice, and competence in digital health. (BCS)
EX-B10-04 — NHS Digital Academy statement that its mission is to empower all NHS staff to develop digital skills needed for healthcare services. (NHS England Workforce)
EX-B10-05 — NHS England warning that staff may face dismissal or prison for inappropriate patient-record access. (NHS England)
EX-B10-06 — Copilot workplace research stressing the need for context-sensitive implementation, role-specific training, and governance for sustainable generative-AI adoption. (arXiv)
Final Breach Position
This breach records that NHS AI deployment creates a competence gap where staff are expected to use, verify, govern, and be accountable for AI-mediated outputs before the public record visibly proves that role-specific training, AI literacy, equality-adjusted support, disciplinary boundaries, and tribunal-safe evidence rules are in place.
Core line:
Training must precede exposure, and competence must precede liability.
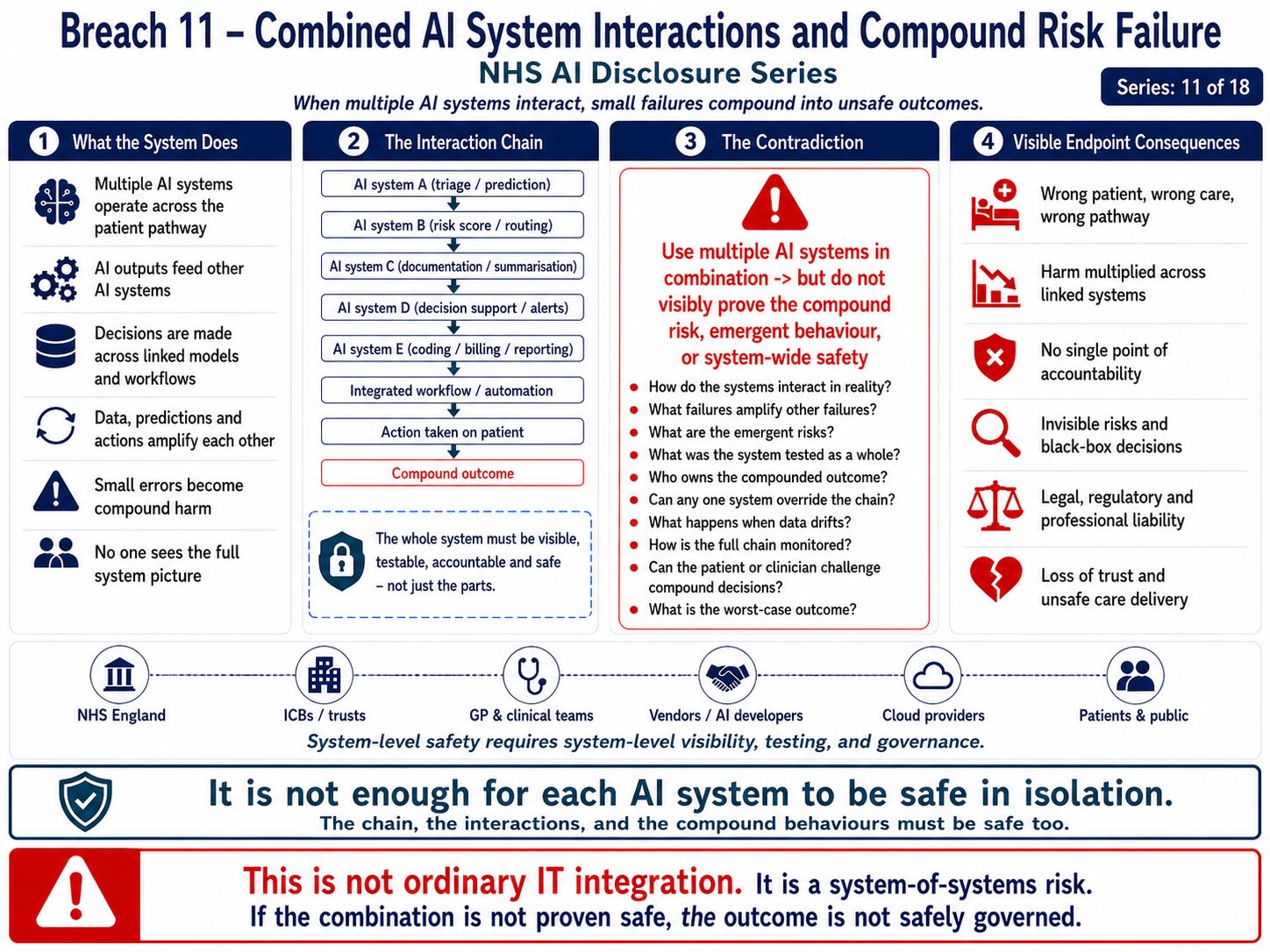
Breach 11 — Clinical Safety Case, DPIA, Equality Impact, and Assurance Visibility Failure. This figure shows how NHS AI systems can affect patient pathways, clinical documentation, workflow, access decisions, audit trails, and safety outcomes before the public record visibly proves the clinical safety case, DPIA, equality impact assessment, hazard log, residual-risk controls, monitoring route, and accountability framework. The breach is the deployment or scaling of AI-mediated healthcare systems before lawful assurance evidence is publicly visible, testable, and connected to the full processing chain.
Breach XI — Clinical Safety Case, DPIA, Equality Impact, and Assurance Visibility Failure
Summary
This breach concerns the absence of visibly published assurance evidence for NHS AI systems being deployed into patient-access, triage, ambient voice, clinical documentation, staff workflow, and cloud / SaaS processing environments.
The breach is not merely that risk assessments may be incomplete.
The breach is that national AI deployment is being publicly advanced before the public record visibly shows the full assurance stack:
- clinical safety case;
- hazard log;
- clinical risk assessment;
- Data Protection Impact Assessment;
- Equality Impact Assessment;
- accessibility assessment;
- algorithmic transparency record
- model assurance;
- technical documentation;
- human oversight plan;
- red-flag testing;
- bias testing;
- post-deployment monitoring;
- incident route;
- and public accountability route.
The breach mechanism is:
AI deployment → patient / staff impact → clinical, data, equality and procedural risk → missing visible assurance evidence → unsafe public-sector deployment posture
Core line:
AI rollout cannot lawfully outrun assurance.
Evidence Supported
NHS England announced that AI triage in the NHS App and widespread access to AI note-taking tools are being prioritised across England as part of a major technology, digital and data overhaul. (NHS England)
NHS England’s clinical-risk guidance states that DCB0129 is designed to help manufacturers of health IT software evidence the clinical safety of their products. (NHS England Digital)
NHS England’s digital clinical safety assurance guidance identifies DCB0160 as the standard for deployment and use of health IT systems, designed to help health and care organisations assure clinical safety. (NHS England)
NHS Digital’s clinical risk management page states that compliance with DCB0129 and DCB0160 is mandatory under the Health and Social Care Act 2012. (NHS England Digital)
The Digital Technology Assessment Criteria covers the core standards, policies and best practice required for use in NHS and adult social care across five areas: clinical safety, data protection, technical security, interoperability, and usability/accessibility. (NHS Transformation Directorate)
The UK Algorithmic Transparency Recording Standard enables public-sector bodies to publish information about algorithmic tools they use and why they use them, with the public-sector guidance explaining that it supports openness about algorithmic tools and algorithm-assisted decisions. (GOV.UK)
Together, these sources support the breach position:
NHS AI systems are being advanced into patient and staff pathways, while the visible public record must show the assurance evidence that makes such deployment lawful, safe, auditable, equal, and accountable.
Mechanism Identified
The mechanism is:
AI system selected → patient / worker pathway affected → software produces output → output influences access, record, workflow, audit or liability → assurance evidence required before safe deployment
The assurance failure arises where public deployment materials describe benefit, speed, productivity, savings, or national rollout, but do not visibly disclose:
- the clinical safety case;
- the hazard log;
- the clinical risk management file;
- the DPIA;
- the Equality Impact Assessment;
- the accessibility assessment;
- the algorithmic transparency record;
- the model documentation;
- the red-flag testing evidence;
- the under-triage testing evidence;
- the accent / language / disability testing evidence;
- the cybersecurity assessment;
- the data-execution map;
- the transfer risk assessment;
- and the post-market monitoring route.
For AI in healthcare, assurance is not an administrative appendix.
Assurance is the legal bridge between deployment and lawful use.
Legal Frameworks Engaged
This breach engages, at minimum:
- Health and Social Care Act 2012 — basis for mandatory clinical risk standards where applicable.
- DCB0129 — clinical risk management for manufacturers of health IT systems.
- DCB0160 — clinical risk management for deploying health and care organisations.
- DTAC — clinical safety, data protection, technical security, interoperability, usability and accessibility.
- UK GDPR Article 5(1)(a) — lawfulness, fairness, transparency.
- UK GDPR Article 5(1)(b) — purpose limitation.
- UK GDPR Article 5(1)(c) — data minimisation.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 6 — lawful basis.
- UK GDPR Article 9 — special-category health data.
- UK GDPR Article 13 — information to data subjects.
- UK GDPR Article 14 — information where data is generated or obtained indirectly.
- UK GDPR Article 15 — right of access.
- UK GDPR Article 16 — rectification.
- UK GDPR Article 21 — right to object.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 28 — processor obligations.
- UK GDPR Article 30 — records of processing activities.
- UK GDPR Article 32 — security of processing.
- UK GDPR Article 35 — Data Protection Impact Assessment.
- UK GDPR Articles 44–49 — transfer safeguards where non-UK execution, support, telemetry or sub-processing exists.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality.
- Caldicott Principles.
- NHS Constitution — safe care, privacy, confidentiality, dignity, informed involvement, non-discriminatory access.
- Equality Act 2010 section 19 — indirect discrimination.
- Equality Act 2010 sections 20–21 — reasonable adjustments.
- Equality Act 2010 section 29 — services and public functions.
- Equality Act 2010 section 149 — Public Sector Equality Duty.
- Accessibility Regulations 2018 — accessibility of public-sector digital services where applicable.
- NHS Accessible Information Standard.
- Human Rights Act 1998 / ECHR Article 8 — medical privacy, bodily autonomy, dignity, private life.
- Human Rights Act 1998 / ECHR Article 14 — non-discrimination.
- Common law negligence / duty of care — foreseeable harm from unsafe software deployment.
- Duty of candour where AI-related harm or near-miss arises.
- Public law rationality, proportionality and procedural fairness.
- Algorithmic Transparency Recording Standard.
- EU AI Act Article 9 — risk management.
- EU AI Act Article 10 — data and data governance.
- EU AI Act Article 11 — technical documentation.
- EU AI Act Article 12 — record keeping / logs.
- EU AI Act Article 13 — transparency and provision of information.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness and cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- EU AI Act Article 50 — AI interaction / generated-output transparency where applicable.
- UNESCO Bioethics Article 5 — autonomy and individual responsibility.
- UNESCO Bioethics Article 6 — consent.
- UNESCO Bioethics Article 9 — privacy and confidentiality.
- UNESCO Bioethics Article 10 — equality, justice and equity.
- ICCPR Article 17 — privacy protection.
- ICESCR Article 12 — right to health.
- UN Guiding Principles on Business and Human Rights — adverse human-rights impact prevention.
Legal Duty
NHS England, ICBs, NHS trusts, GP practices, vendors, processors, and deploying organisations must demonstrate that AI systems affecting patient access, clinical documentation, staff workflow, or medical data processing have been assessed before deployment.
That duty includes producing and maintaining:
- a clinical safety case;
- a hazard log;
- a clinical risk management file;
- a DPIA;
- an Equality Impact Assessment;
- an accessibility assessment;
- an algorithmic transparency record;
- a model / system technical description;
- a data-flow and execution map;
- a processor / sub-processor map;
- a human oversight plan;
- an incident response route;
- a correction and rectification route;
- a patient objection route;
- a staff training route;
- a post-deployment monitoring plan;
- and an evidence trail showing that foreseeable risks have been assessed.
Where AI affects clinical access or patient records, assurance must precede deployment.
Breach Identified
The breach identified is the absence of visible public assurance evidence sufficient to justify national AI deployment into healthcare access and documentation pathways.
The public record shows deployment momentum.
It does not visibly show, for each AI system:
clinical safety case → DPIA → equality impact → accessibility test → algorithmic transparency record → model assurance → data execution map → post-deployment monitoring
That missing assurance stack is a breach because these AI systems are not neutral back-office utilities.
They may affect:
- whether a patient is routed to GP, pharmacy, A&E, self-care, or community service;
- whether a patient is delayed;
- whether a symptom is under-triaged;
- whether a consultation is correctly captured;
- whether an AI summary enters the medical record;
- whether staff are audited;
- whether logs become disciplinary material;
- whether patient data crosses execution environments;
- whether protected groups face unequal error rates;
- and whether patients have meaningful routes to object, correct, or challenge.
That requires visible assurance.
Clinical Safety Failure Risk
Clinical safety is not optional where software affects care pathways.
If the AI system contributes to triage, routing, documentation, clinical summaries, appointment allocation, or record formation, the safety case must identify:
- hazards;
- harms;
- severity;
- likelihood;
- mitigations;
- residual risk;
- clinical safety officer responsibility;
- human oversight;
- escalation thresholds;
- under-triage controls;
- false reassurance controls;
- red-flag symptoms;
- post-deployment monitoring;
- and incident reporting.
Without that, public deployment relies on claimed benefit rather than risk-governed safety.
DPIA Failure Risk
A DPIA is required where processing is likely to result in a high risk to rights and freedoms.
NHS AI triage, ambient voice, Copilot-style tools, voice transcription, clinical summaries, patient-access routing, prompt logging, telemetry, and model monitoring all raise high-risk processing indicators because they involve:
- special-category health data;
- possible large-scale processing;
- vulnerable data subjects;
- new technology;
- possible automated or semi-automated decision support;
- profiling / pattern analysis;
- cloud and sub-processor chains;
- and patient access consequences.
The DPIA must assess execution, not just storage.
Equality Impact Failure Risk
Equality assessment is required because AI systems may perform differently across:
- accent;
- language;
- disability;
- age;
- race / ethnicity;
- nationality / migrant background;
- digital literacy;
- poverty;
- device access;
- neurodivergence;
- and health literacy.
The Sussex pilot issue is one example.
If the system has not been tested across high-diversity regions and populations, a national rollout may produce unequal access and unequal error rates.
Algorithmic Transparency Failure Risk
The Algorithmic Transparency Recording Standard exists so public bodies can explain how and why algorithmic tools are being used. It is not enough to publish broad claims of “AI support” or “digital transformation.”
For NHS AI systems, algorithmic transparency should identify:
- the system name;
- the purpose;
- the decision or process supported;
- the organisation using it;
- the vendor;
- the data used;
- the output generated;
- human oversight;
- risk mitigation;
- review process;
- and routes for challenge or redress.
Without that, patients and staff are exposed to opaque public-sector automation.
Tribunal / Procedural Risk
This breach has tribunal and procedural relevance because assurance documents may become necessary evidence.
In employment, tribunal, regulatory, data-protection, clinical-negligence, judicial-review, coronial, or public-law proceedings, the following may need to be disclosed:
- safety case;
- DPIA;
- equality assessment;
- algorithmic transparency record;
- risk register;
- model version;
- audit log;
- training record;
- incident record;
- human-review policy;
- data-flow map;
- processing-location map;
- and vendor / sub-processor list.
Where such assurance is missing, incomplete, or not disclosed, the affected party cannot fairly test the lawfulness, safety, accuracy, or reliability of the AI system.
Disclosure Questions
- What clinical safety case exists for AI triage?
- What DCB0129 manufacturer file exists?
- What DCB0160 deployment file exists?
- Who is the clinical safety officer?
- What hazard log exists?
- What under-triage hazards were identified?
- What false reassurance hazards were identified?
- What ambient voice record-error hazards were identified?
- What Copilot patient-data hazards were identified?
- What residual risk was accepted?
- Who accepted the residual risk?
- What DPIA exists for AI triage?
- What DPIA exists for ambient voice?
- What DPIA exists for Copilot-style staff tools?
- Does the DPIA identify execution location?
- Does the DPIA identify logs and telemetry?
- Does the DPIA identify model improvement use?
- Does the DPIA identify cross-border data bleed?
- What Equality Impact Assessment exists?
- What accent / dialect / language testing was included?
- What disability testing was included?
- What age and digital-exclusion testing was included?
- What accessibility assessment exists?
- What DTAC assessment exists?
- What Algorithmic Transparency Record exists?
- What technical documentation identifies the model or engine?
- What public document identifies human oversight?
- What post-deployment monitoring exists?
- What incident reporting route exists?
- What evidence proves assurance preceded deployment?
Evidence Relied Upon
EX-B11-01 — NHS England announcement prioritising AI triage in the NHS App and widespread access to AI note-taking tools across England. (NHS England)
EX-B11-02 — NHS England DCB0129 standard page stating the standard helps manufacturers of health IT software evidence clinical safety. (NHS England Digital)
EX-B11-03 — NHS England digital clinical safety assurance page identifying DCB0160 as the deployment and use standard for clinical risk management. (NHS England)
EX-B11-04 — NHS Digital clinical risk management standards page stating DCB0129 and DCB0160 compliance is mandatory under the Health and Social Care Act 2012. (NHS England Digital)
EX-B11-05 — Digital Technology Assessment Criteria guidance stating DTAC covers clinical safety, data protection, technical security, interoperability, usability and accessibility. (NHS Transformation Directorate)
EX-B11-06 — UK Algorithmic Transparency Recording Standard guidance explaining public-sector publication of algorithmic tools and why they are used. (GOV.UK)
EX-B11-07 — Algorithmic Transparency Recording Standard Hub stating algorithmic transparency means being open about how algorithmic tools support decisions in complete, understandable and accessible form. (GOV.UK)
EX-B11-08 — Research proposing an NHS explainability-enabled clinical safety framework, noting that AI’s probabilistic and adaptive behaviour creates assurance questions for existing DCB0129 / DCB0160 safety cases. (arXiv)
Final Breach Position
This breach records that NHS AI deployment cannot be justified through public benefit claims alone.
Where AI systems affect patient access, clinical documentation, staff workflow, audit trails, or medical data processing, the public body must be able to show the assurance stack.
Until clinical safety, DPIA, equality, accessibility, algorithmic transparency, model assurance, and monitoring evidence are visible, the deployment remains legally and clinically unresolved.
Core line:
A national AI rollout without visible assurance is not innovation. It is unmanaged public-sector risk.
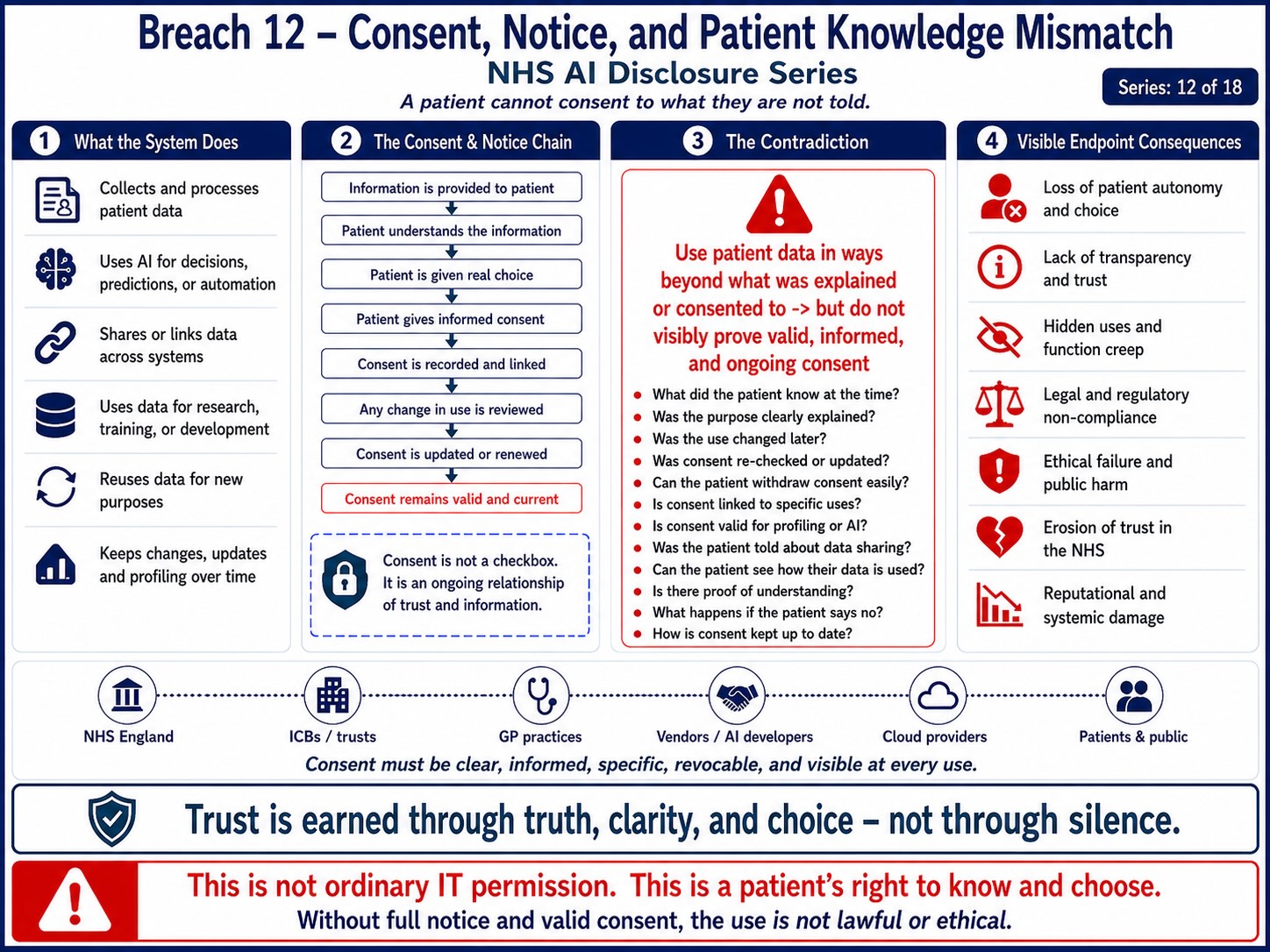
Breach 12 — Patient Access Inequality and Digital Exclusion. This figure shows how AI-mediated access can reshape NHS entry points through apps, portals, automated triage, speech systems, digital forms, and online routing before the public record proves that digitally excluded patients can still access care safely and equally. The breach is the scaling of AI access pathways before equality, accessibility, disability, language, age, poverty, device-access, literacy, and human fallback safeguards are visibly tested, disclosed, and governed.
Breach XII — Patient Access Inequality and Digital Exclusion
Summary
This breach concerns the risk that NHS AI triage, NHS App routing, digital-first access, ambient voice systems, automated booking, and AI-mediated patient pathways create unequal access to care for patients who cannot use, trust, understand, or safely rely on digital and AI systems.
The breach is not simply that the NHS is modernising.
The breach is that AI-mediated access may become a practical gatekeeping layer before the public record visibly proves that non-digital, non-AI, accessible, language-supported, disability-adjusted, and human-reviewed alternatives remain equally available.
The breach mechanism is:
patient needs care → digital / AI route becomes default → patient faces device, literacy, disability, language, poverty, age, trust, speech, or access barrier → delayed or unequal care → health inequality worsens
Core line:
Digital access is not equal access if the excluded patient reaches care later.
Evidence Supported
NHS England states that the NHS App’s new AI triage tool is being rolled out after a successful trial, with expected reach to more than 200,000 patients within 12 months and availability to all NHS App users by April 2028. (NHS England)
Public reporting describes the NHS App AI tool as triaging patients and advising whether they should receive a GP appointment, attend a pharmacy, attend A&E, or use another service route. (The Guardian)
NHS England’s own digital-inclusion framework states that digital exclusion can compound health inequalities by increasing barriers to accessing healthcare, skills, capability, and resources needed to lead a healthy life. (NHS England)
The NHS Accessible Information Standard states that NHS and publicly funded adult social care providers must ensure that disabled people and people with sensory loss can access and understand information and receive the communication support they need. (NHS England)
Those sources support the breach position:
AI triage and NHS App access cannot be treated as neutral where digital exclusion and communication barriers are already recognised health-inequality risks.
Mechanism Identified
The mechanism is:
digital route offered → AI triage embedded → patient must navigate app / device / login / questions / language / symptom entry → system produces output → patient follows route or fails to complete process
The inequality risk enters at several points.
1. Device access
A patient may not own a smartphone, may have limited data, may share a device, may lack secure internet, or may be unable to access the NHS App.
2. Login and identity barriers
A patient may struggle with NHS login, password recovery, identity verification, app updates, browser access, or multi-step authentication.
3. Health-literacy barriers
A patient may not understand symptom questions, urgency indicators, red-flag prompts, medical vocabulary, or routing advice.
4. Language and communication barriers
A patient may speak English as an additional language, use non-standard English, need interpretation, use British Sign Language, or require easy-read / accessible communication.
5. Disability barriers
A patient may have visual impairment, hearing impairment, cognitive impairment, learning disability, neurodivergence, dexterity impairment, mental-health distress, or fatigue affecting digital use.
6. Poverty barriers
A patient may have no reliable broadband, limited data, pay-as-you-go phone access, no private space, no printer, no email, or no capacity to wait online.
7. Trust and confidentiality barriers
A patient may avoid digital routes because of domestic abuse, immigration fear, employment fear, coercive control, safeguarding concern, shared-device risk, or distrust of AI processing.
8. Speech and accent barriers
Where voice, ambient capture, or speech-adjacent AI is used, accent, dialect, speech impairment, background noise, or multilingual speech may create unequal error rates.
This is not a marginal concern.
It is a foreseeable access-risk architecture.
Legal Frameworks Engaged
This breach engages, at minimum:
- Equality Act 2010 section 19 — indirect discrimination.
- Equality Act 2010 sections 20–21 — reasonable adjustments.
- Equality Act 2010 section 29 — services and public functions.
- Equality Act 2010 section 149 — Public Sector Equality Duty.
- NHS Accessible Information Standard / DAPB1605.
- Public Sector Bodies Accessibility Regulations 2018.
- Human Rights Act 1998 / ECHR Article 8 — private life, dignity, bodily autonomy, medical privacy.
- Human Rights Act 1998 / ECHR Article 14 — non-discrimination in enjoyment of rights.
- UK GDPR Article 5(1)(a) — lawfulness, fairness, transparency.
- UK GDPR Article 5(1)(c) — data minimisation.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 6 — lawful basis.
- UK GDPR Article 9 — special-category health data.
- UK GDPR Article 13 — patient-facing information.
- UK GDPR Article 15 — access rights.
- UK GDPR Article 16 — rectification.
- UK GDPR Article 21 — objection.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 35 — DPIA.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality.
- Caldicott Principles.
- NHS Constitution — access to NHS services, dignity, respect, informed involvement, confidentiality.
- Common law negligence / duty of care — foreseeable harm from delayed or unequal access.
- Public law rationality and proportionality.
- Public law procedural fairness.
- Health inequalities duties under NHS / health legislation.
- DCB0129 / DCB0160 clinical safety standards where AI affects patient pathways.
- DTAC usability and accessibility requirements.
- EU AI Act Article 9 — risk management.
- EU AI Act Article 10 — data governance.
- EU AI Act Article 13 — transparency and provision of information.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness and cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- UNESCO Bioethics Article 10 — equality, justice and equity.
- ICESCR Article 12 — right to health.
- UN Guiding Principles on Business and Human Rights — adverse human-rights impact prevention.
Legal Duty
NHS England, ICBs, GP practices, NHS trusts, vendors, and public-sector deployers must ensure that AI-mediated and digital-first access routes do not create unequal access to healthcare.
That duty requires:
- non-digital access routes;
- non-AI access routes;
- telephone alternatives;
- walk-in or assisted routes where clinically necessary;
- interpreter support;
- accessible information;
- easy-read information;
- screen-reader compatibility;
- disability adjustments;
- carer / advocate support;
- safeguards for shared-device users;
- safeguarding-sensitive routes;
- manual override;
- human escalation;
- and monitoring of access outcomes by protected and disadvantaged groups.
The duty is not satisfied by making an app available.
The duty is satisfied only where the patient who cannot use the app is not disadvantaged.
Breach Identified
The breach identified is the risk that AI triage and NHS App routing become the default access layer without visible proof that excluded patients receive equivalent access.
Digital-first design can become exclusion-by-design where the practical route to care depends on:
- owning a device;
- trusting the app;
- understanding the interface;
- answering AI questions correctly;
- reading digital instructions;
- having data or broadband;
- navigating login;
- speaking standard English;
- and accepting AI processing.
That is not universal healthcare access.
That is conditional digital access.
The breach arises if patients who are digitally excluded, disabled, poor, older, language-diverse, neurodivergent, visually impaired, hearing impaired, cognitively impaired, or safeguarding-vulnerable are required to pass through a more difficult route before reaching care.
Health Inequality Risk
NHS England recognises that digital exclusion can compound health inequalities. (NHS England)
That means the risk is already institutionally known.
Where the NHS then deploys AI triage through the NHS App, it must show how that known risk has been mitigated.
The inequality chain is:
known digital exclusion → AI triage placed into access route → vulnerable patient faces higher friction → delayed or misdirected care → inequality worsens
This is a governance failure if not assessed before rollout.
Accessibility and Communication Risk
The Accessible Information Standard requires NHS and adult social care organisations to ensure that people with disability, impairment or sensory loss can access and understand information and receive communication support. (NHS England)
AI triage raises specific accessible-information questions:
- Are questions screen-reader compatible?
- Are outputs available in accessible formats?
- Are red-flag warnings clear?
- Is easy-read available?
- Is BSL support available?
- Is interpreter support available?
- Can carers assist without compromising confidentiality?
- Can disabled patients bypass AI where needed?
- Are reasonable adjustments built into the route?
If the system cannot answer those questions, it cannot safely claim equal access.
Patient-Access Risk
The patient-access risk chains include:
older patient without app confidence → avoids AI triage → delays contacting GP → condition worsens
disabled patient cannot understand or complete AI questions → system gives incomplete output → wrong route
patient with limited English misunderstands symptom question → system under-triages
patient using shared phone cannot disclose sensitive symptom → incomplete data entered → wrong triage
patient under coercive control cannot safely use app → digital route becomes unsafe
patient with no data credit cannot complete digital triage → falls back into phone queue or no care
These are foreseeable, not exceptional.
Tribunal / Procedural Risk
This breach also has tribunal and procedural relevance.
AI access inequality may later arise in:
· disability discrimination claims;
· reasonable-adjustment disputes;
· judicial review;
· data-protection complaints;
· clinical negligence claims;
· protected-disclosure claims;
· employment disputes involving staff required to enforce digital pathways;
· and complaints about delayed or unequal care.
Where unequal access is alleged, the following evidence may be required:
- Equality Impact Assessment;
- accessibility test results;
- DPIA;
- digital inclusion assessment;
- user research by protected group;
- app completion rates by demographic group;
- abandonment rates;
- telephone fallback rates;
- urgent-care misrouting rates;
- interpreter availability;
- reasonable-adjustment logs;
- and complaint / incident data.
Without that evidence, the public body cannot demonstrate equal access.
Disclosure Questions
- What Equality Impact Assessment covers NHS App AI triage?
- What digital inclusion assessment covers AI triage?
- What accessibility assessment covers AI triage?
- What DPIA covers digitally excluded patients?
- What non-digital route remains available?
- What non-AI route remains available?
- Is telephone access equivalent?
- Is assisted access available?
- Can patients bypass AI triage?
- Can patients use GP reception without disadvantage?
- Are older patients specifically tested?
- Are disabled patients specifically tested?
- Are visually impaired patients tested?
- Are hearing-impaired patients tested?
- Are patients with learning disabilities tested?
- Are neurodivergent patients tested?
- Are patients with limited English tested?
- Are patients without smartphones tested?
- Are patients without broadband or data tested?
- Are shared-device risks assessed?
- Are domestic-abuse and coercive-control risks assessed?
- Are safeguarding-sensitive conditions assessed?
- Are sexual health, mental health, immigration-sensitive, employment-sensitive, and domestic-abuse disclosures protected?
- Are app abandonment rates monitored?
- Are AI triage completion rates monitored by demographic group?
- Are misrouting rates monitored by protected group?
- Are under-triage rates monitored by protected group?
- Are complaint rates monitored by access route?
- What reasonable-adjustment pathway exists?
- What evidence proves equal access is preserved?
Evidence Relied Upon
EX-B12-01 — NHS England announcement that the NHS App AI triage tool is being rolled out to more than 200,000 patients within 12 months and all NHS App users by April 2028. (NHS England)
EX-B12-02 — Public reporting describing NHS App AI triage as advising patients whether they should receive a GP appointment, attend pharmacy, attend A&E, or use another route. (The Guardian)
EX-B12-03 — NHS England inclusive digital healthcare framework stating that digital exclusion can compound health inequalities by increasing barriers to healthcare access and digital capability. (NHS England)
EX-B12-04 — NHS Accessible Information Standard implementation guidance stating that people with disability, impairment or sensory loss must be able to access and understand information and receive needed communication support. (NHS England)
EX-B12-05 — NHS England Accessible Information Standard publication page confirming the standard’s purpose and update status. (NHS England)
Final Breach Position
This breach records that AI triage and digital-first NHS access cannot be treated as universal access merely because they are available through the NHS App.
Universal healthcare requires equivalent access for the patient who cannot use, understand, trust, afford, or safely disclose through the AI route.
Until NHS England shows the equality, accessibility, digital-inclusion, reasonable-adjustment, and non-AI fallback architecture, AI triage creates unresolved health-inequality risk.
Core line:
A digital front door is still a closed door for the patient who cannot open it.
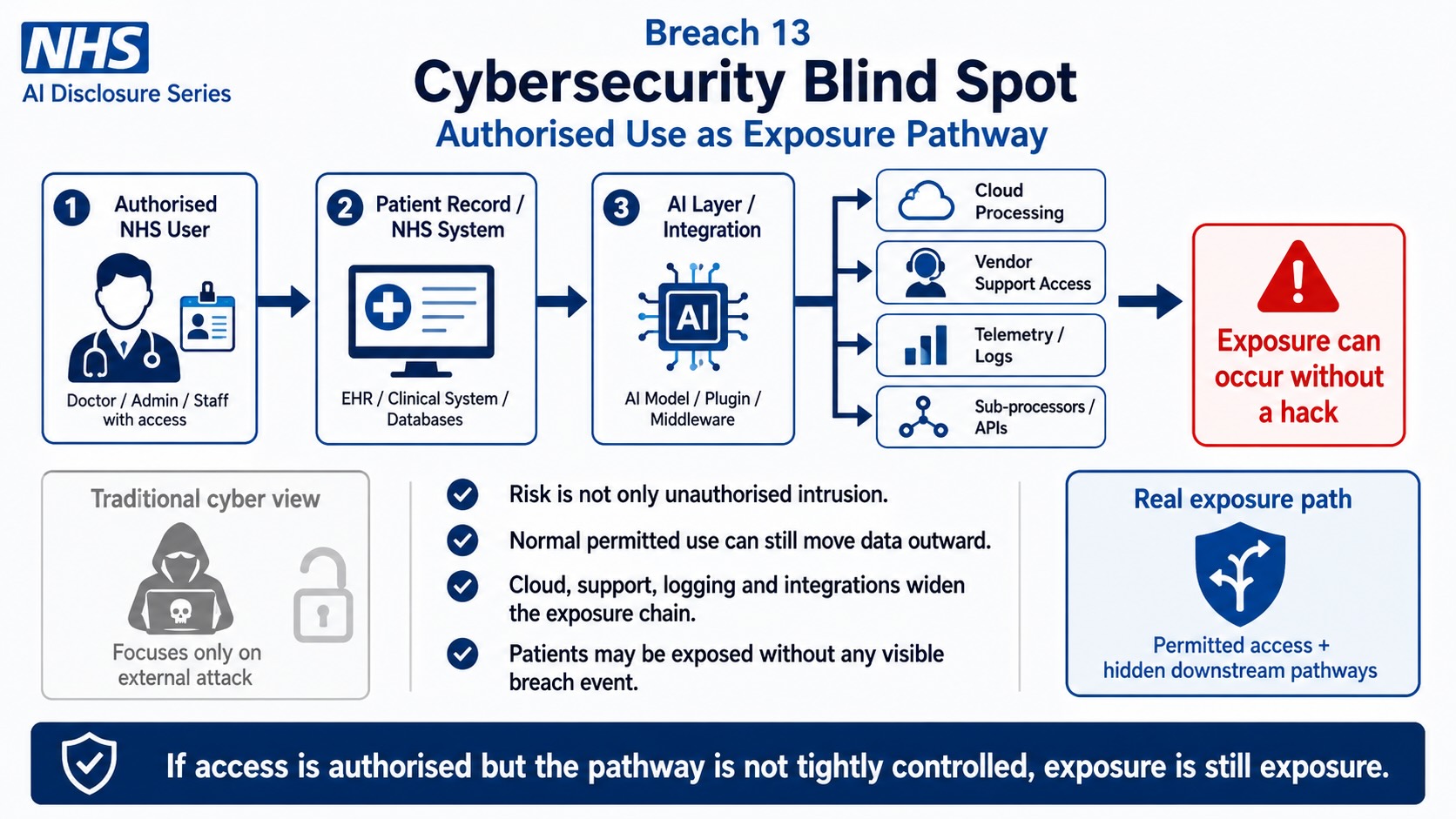
Breach 13 — Cybersecurity Blind Spot: Authorised Use as Exposure Pathway. This figure shows how exposure can occur through authorised NHS access when patient records pass into AI layers, cloud processing, vendor support access, telemetry, logs, sub-processors, APIs, and downstream integrations. The breach is the treatment of cybersecurity as only an external hacking problem before the public record proves that permitted access, logging, support routes, integrations, and hidden outbound pathways are tightly controlled and transparently governed.
Breach XIII — Cybersecurity Blind Spot: Authorised Use as Exposure Pathway
Summary
This breach concerns the mistaken assumption that NHS AI cybersecurity risk is mainly about external hacking, ransomware, or unauthorised intrusion.
The breach is broader.
AI systems create exposure through authorised use.
That means risk may arise even where every user is logged in, every licence is valid, every system is approved, every access event is authenticated, and every action appears procedurally normal.
The breach mechanism is:
authorised NHS user → approved AI / SaaS tool → patient or staff data processed → prompt / output / log / telemetry / audit / support event generated → exposure occurs inside normal system operation
This is the cybersecurity blind spot.
Traditional cybersecurity asks:
Was there unauthorised access?
AI-era healthcare security must also ask:
What does authorised processing expose?
Core line:
The breach is not only the hacker outside the system. The breach may be the approved pathway inside the system.
Evidence Supported
NHS AI deployment expands the number of approved digital routes through which patient data, staff data, clinical text, voice data, symptom input, workflow content, prompts, outputs, audit trails, and telemetry may be processed.
This includes:
- AI triage;
- NHS App patient routing;
- ambient voice technology;
- AI scribing;
- Copilot-style staff tools;
- clinical summarisation;
- SaaS triage platforms;
- cloud-hosted processing;
- GP system integration;
- staff audit trails;
- vendor support;
- processor / sub-processor access;
- logging;
- analytics;
- and model monitoring.
The supported exposure route is therefore:
patient / staff data enters an approved AI pathway → the pathway itself creates secondary data exhaust → that exhaust may carry clinical, behavioural, identity, or workflow meaning
That is not ordinary database breach logic.
It is authorised-processing exposure.
Mechanism Identified
The mechanism is:
authorised access → AI processing → system exhaust → secondary exposure
1. Authorised access
A staff member, clinician, administrator, patient, vendor, support worker, or system service account may lawfully access or process information.
2. AI processing
The approved tool may summarise, classify, transcribe, retrieve, generate, route, recommend, prioritise, log, or analyse.
3. System exhaust
The AI system may create:
- prompts;
- generated outputs;
- transcripts;
- summaries;
- confidence scores;
- routing decisions;
- access logs;
- telemetry;
- audit events;
- model-performance records;
- diagnostic logs;
- support tickets;
- error reports;
- crash reports;
- analytics;
- monitoring events;
- security alerts;
- and improvement signals.
4. Secondary exposure
Those secondary records may reveal:
- patient identity;
- clinical condition;
- symptom pattern;
- staff behaviour;
- workflow pattern;
- treatment pathway;
- urgency classification;
- disability status;
- protected disclosure;
- complaint history;
- or employment-risk material.
The exposure is not created by an attacker.
It is created by the authorised system design.
Legal Frameworks Engaged
This breach engages, at minimum:
- UK GDPR Article 5(1)(a) — lawfulness, fairness and transparency.
- UK GDPR Article 5(1)(b) — purpose limitation.
- UK GDPR Article 5(1)(c) — data minimisation.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(e) — storage limitation.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 6 — lawful basis.
- UK GDPR Article 9 — special-category health data.
- UK GDPR Article 13 — transparency where data is collected from patients or staff.
- UK GDPR Article 14 — transparency where data is generated indirectly through logs, analytics, telemetry, or derived records.
- UK GDPR Article 15 — right of access.
- UK GDPR Article 16 — rectification.
- UK GDPR Article 18 — restriction of processing.
- UK GDPR Article 21 — right to object.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 28 — processor obligations.
- UK GDPR Article 30 — records of processing activities.
- UK GDPR Article 32 — security of processing.
- UK GDPR Article 33 — personal data breach notification to supervisory authority where applicable.
- UK GDPR Article 34 — communication of personal data breach to data subject where applicable.
- UK GDPR Article 35 — Data Protection Impact Assessment.
- UK GDPR Articles 44–49 — international transfers where logs, support, telemetry, analytics, or processing cross borders.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality.
- Caldicott Principles.
- NHS Constitution — privacy, confidentiality, dignity, safe care.
- NHS Records Management Code of Practice.
- Human Rights Act 1998 / ECHR Article 8 — medical privacy, private life, dignity, psychological integrity.
- Human Rights Act 1998 / ECHR Article 14 — non-discrimination where cybersecurity exposure affects protected groups unevenly.
- Equality Act 2010 section 149 — Public Sector Equality Duty.
- Health and Safety at Work etc. Act 1974 section 2 — staff safety where system ambiguity creates stress or liability exposure.
- Management of Health and Safety at Work Regulations 1999 — risk assessment.
- Employment Rights Act 1996 section 47B — detriment for protected disclosure where staff raise AI/security concerns.
- Employment Rights Act 1996 section 103A — dismissal for protected disclosure.
- Public Interest Disclosure Act 1998.
- Public law rationality, proportionality and transparency.
- DCB0129 / DCB0160 clinical safety standards where exposure affects clinical software or pathways.
- DTAC technical security requirements.
- EU AI Act Article 9 — risk management.
- EU AI Act Article 10 — data and data governance.
- EU AI Act Article 11 — technical documentation.
- EU AI Act Article 12 — record keeping / logs.
- EU AI Act Article 13 — transparency and provision of information.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness and cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- Convention 108+ — data protection safeguards.
- OECD Privacy Guidelines — security safeguards, use limitation, accountability.
- UN Guiding Principles on Business and Human Rights — prevention of adverse rights impacts through business systems.
Legal Duty
NHS England, ICBs, NHS trusts, GP practices, vendors, processors, sub-processors, cloud providers, and deploying organisations must assess cybersecurity beyond unauthorised access.
They must assess:
- authorised-user risk;
- prompt leakage;
- output leakage;
- log exposure;
- telemetry exposure;
- support-access exposure;
- audit-trail exposure;
- model-monitoring exposure;
- analytics exposure;
- debugging exposure;
- crash-report exposure;
- staff surveillance risk;
- patient re-identification risk;
- role-permission mismatch;
- system-service account access;
- vendor administrator access;
- and insider risk created by normal operation.
The legal duty is not satisfied by saying the system is secure from external attack.
The system must also be safe in ordinary use.
Breach Identified
The breach identified is the apparent cybersecurity blind spot created where AI systems are treated as secure because they are approved, authenticated, hosted, contracted, or encrypted.
That is incomplete.
AI systems can expose sensitive information without a hack.
Examples include:
- a prompt containing patient information;
- a generated summary containing identifiable clinical detail;
- a transcript containing third-party family information;
- a log retaining symptom data;
- telemetry recording behavioural access patterns;
- an audit trail identifying staff conduct;
- an error report containing clinical text;
- a support ticket containing screenshots or copied data;
- a model-monitoring record containing red-flag classification;
- a dashboard showing small-cohort patterns;
- or a debugging trace revealing patient workflow.
All of these can arise through authorised system use.
That is the breach.
Authorised-Use Exposure Pathways
1. Prompt exposure
Staff may enter patient-adjacent information into AI tools. Even where this is permitted or technically possible, the prompt may itself become a stored record, audit item, or telemetry event.
2. Output exposure
Generated outputs may contain patient data, inferred conditions, summaries, triage routes, or staff-relevant content. Outputs may be retained, copied, exported, inserted into records, or used in later proceedings.
3. Log exposure
Access logs, model logs, audit logs, and security logs may reveal clinical or behavioural meaning even where the original content is not visible.
4. Telemetry exposure
Telemetry may record system use, performance, patterns, errors, classifications, latency, user behaviour, workflow intensity, or interaction metadata.
5. Support exposure
Vendor or sub-processor support teams may receive data through tickets, screenshots, diagnostics, error traces, or system-level access.
6. Debugging exposure
Debugging often requires enough operational context to reproduce or diagnose failure. In healthcare AI, that context may include clinical content or patient-pathway data.
7. Model-monitoring exposure
Model performance monitoring may record wrong outputs, overrides, red-flag cases, under-triage events, or unusual symptom clusters.
8. Staff-surveillance exposure
Named-user AI tools can create behavioural profiles of staff use, productivity, prompts, retrievals, edits, and compliance patterns.
These are cybersecurity issues even when no criminal attacker exists.
Patient-Data Risk
The patient-data risk chain is:
patient symptom / voice / record data → AI processing → prompt / log / telemetry / support record → secondary record retains clinical meaning → exposure risk persists outside the original care context
This creates a purpose-limitation problem.
The patient gave information for care.
The system may generate additional records for:
- monitoring;
- audit;
- debugging;
- security;
- vendor support;
- analytics;
- product improvement;
- performance reporting;
- or staff management.
Those secondary purposes must be lawful, necessary, proportionate, transparent, and minimised.
Staff-Data Risk
The staff-data risk chain is:
named user → AI tool use → prompts / outputs / retrievals / corrections / overrides logged → behaviour profile created → performance, disciplinary, audit, or tribunal use becomes possible
That creates employment and data-protection risk.
The staff member may not understand that AI use generates a secondary evidential record.
This links directly to:
· Breach I — criminal-threat governance;
· Breach II — named-user licence exposure;
· Breach X — training and competence mismatch.
Sovereignty and Cross-Border Risk
Authorised-use exposure also creates sovereignty risk.
Even where the main database is UK-hosted, secondary records may be processed through:
- support systems;
- telemetry platforms;
- cloud monitoring;
- security tooling;
- analytics services;
- vendor ticketing systems;
- diagnostic pipelines;
- backup environments;
- disaster recovery;
- and model-performance systems.
This means cross-border exposure may occur not through the clinical database, but through the operational exhaust of the AI system.
Core line:
The clinical database may stay in the UK while the meaning of the data leaks through logs.
Tribunal / Procedural Risk
This breach has direct procedural relevance because authorised-use records may later become evidence.
In disciplinary, employment tribunal, whistleblowing, data-protection, clinical-negligence, regulatory, or judicial-review proceedings, AI cybersecurity records may include:
- prompts;
- access logs;
- generated outputs;
- user activity records;
- telemetry;
- audit events;
- support tickets;
- system alerts;
- incident reports;
- override histories;
- correction records;
- and model-monitoring records.
If those records are relied upon, the affected party must be able to test:
- whether the record was user-generated or system-generated;
- whether the record is complete;
- whether it contains derived or inferred data;
- whether it was altered by normalisation;
- whether it was generated automatically;
- whether it was seen by the worker;
- whether it was accurate;
- whether it was retained lawfully;
- whether it was shared with vendors;
- and whether it was processed outside the UK.
Without that evidence chain, the record may be procedurally unsafe.
Disclosure Questions
- What authorised-use exposure assessment has been completed for NHS AI systems?
- Are prompts treated as patient data where they contain clinical content?
- Are AI outputs treated as patient data where they contain clinical content?
- Are logs treated as patient data where they reveal clinical meaning?
- Are telemetry records treated as personal data?
- Are model-monitoring records treated as personal data?
- Are staff prompts retained?
- Are patient symptom prompts retained?
- Are outputs retained?
- Are transcripts retained?
- Are summaries retained?
- Are audit logs linked to named staff users?
- Are support tickets screened for patient data?
- Are screenshots allowed in vendor support tickets?
- Are error reports redacted before vendor access?
- Are debugging traces minimised?
- Are telemetry records minimised?
- Are logs encrypted separately from clinical records?
- Who can access AI logs?
- Who can access telemetry?
- Who can access support tickets?
- Who can access model-monitoring records?
- Can vendor administrators access patient-adjacent records?
- Can sub-processors access logs or telemetry?
- Are logs or telemetry processed outside the UK?
- Are AI usage records used for staff performance monitoring?
- Are AI usage records used for discipline?
- Are AI usage records used for clinical safety monitoring?
- What breach-notification rule applies to prompt or telemetry exposure?
- What public document identifies authorised-use exposure controls?
Evidence Relied Upon
EX-B13-01 — NHS AI triage deployment materials showing AI is being inserted into patient-access pathways.
EX-B13-02 — NHS ambient voice / AI scribing materials showing AI is being inserted into consultation capture and clinical documentation.
EX-B13-03 — NHS Copilot deployment materials showing staff-facing AI tools are being deployed at mass scale.
EX-B13-04 — NHS data-protection and information-governance materials recognising the need for confidentiality, security, access control, and appropriate handling of patient data.
EX-B13-05 — Cloud / SaaS sub-processor materials showing that NHS digital environments rely on vendors, processors, sub-processors, infrastructure providers, support pathways, and operational services.
EX-B13-06 — UK GDPR Article 32 security-of-processing duty, requiring appropriate security measures for personal data processing.
EX-B13-07 — UK GDPR Article 25 data-protection-by-design duty, requiring privacy and security to be built into the system design, not applied after exposure.
Final Breach Position
This breach records that NHS AI cybersecurity cannot be assessed only through external attack, hacking, encryption, hosting, or authentication.
AI systems create exposure through ordinary authorised use.
Prompts, outputs, transcripts, summaries, logs, telemetry, audit trails, support tickets, debugging records, model-monitoring data, and staff activity records can all carry patient or worker meaning.
Until NHS England and deploying bodies disclose how authorised-use exposure is prevented, minimised, logged, governed, corrected, and contained, the cybersecurity posture remains incomplete.
Core line:
AI cybersecurity fails if it protects the database but ignores the exhaust.
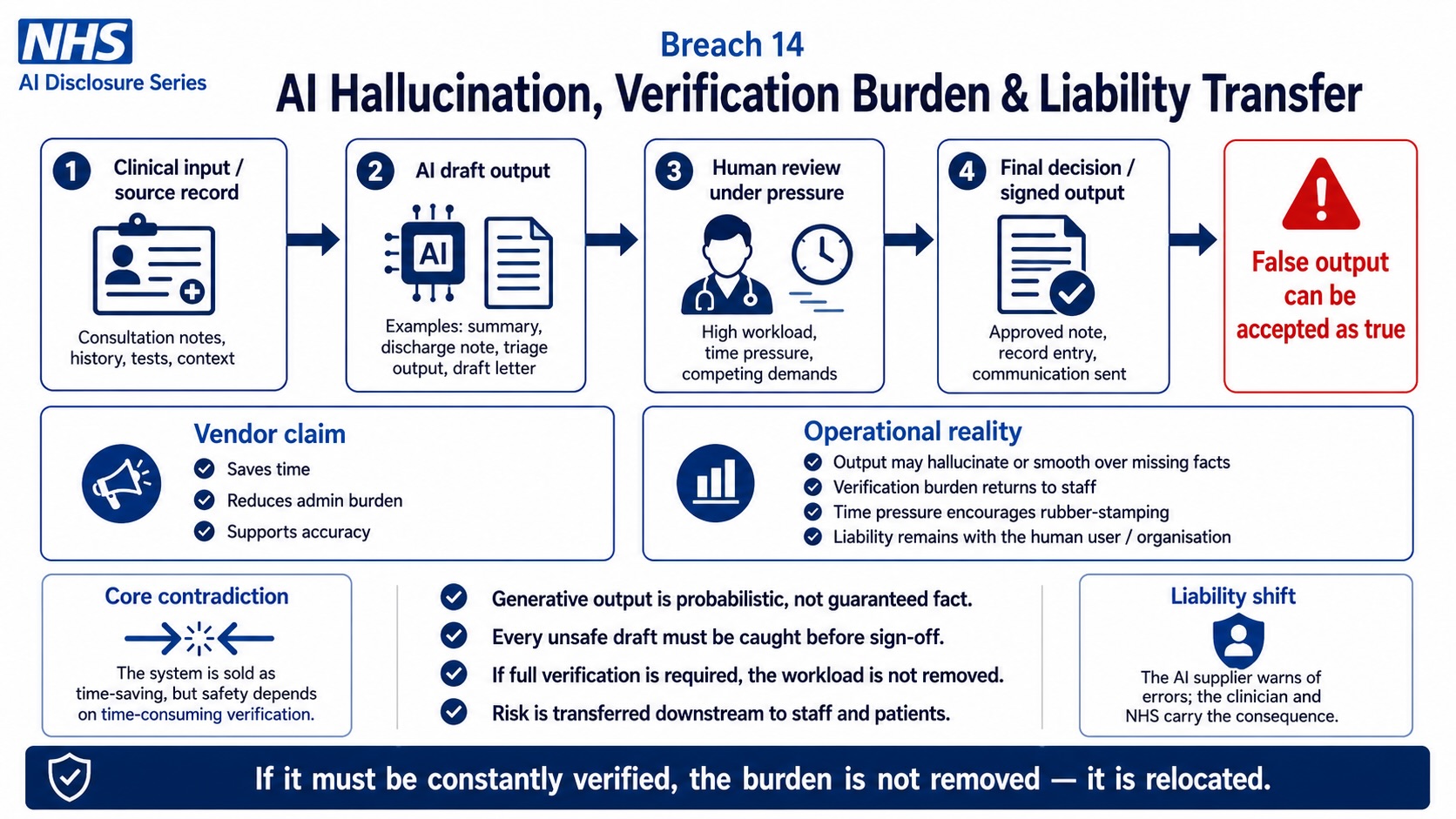
Breach 14 — AI Hallucination, Verification Burden & Liability Transfer. This figure shows how AI-generated draft outputs can move from clinical input into summaries, notes, triage outputs, draft letters, record entries, and communications before their accuracy is fully verified. The breach is the relocation of safety burden onto staff where probabilistic AI output may hallucinate, omit, smooth over, or misstate facts, while human reviewers remain under workload pressure and liability shifts downstream to clinicians, organisations, and patients.
Breach XIV — AI Hallucination, Verification Burden, and Workforce Stress Risk
Summary
This breach concerns the risk that AI-generated outputs create an additional verification burden for NHS staff while being publicly framed as time-saving, productivity-enhancing, or administrative relief.
The breach is not that AI outputs can never be useful.
The breach is that AI tools may produce fluent, confident, plausible outputs that still require human verification, correction, contextual review, clinical judgment, record checking, confidentiality checking, and legal-risk assessment.
That means the claimed time saving may conceal a transferred burden:
AI generates → worker verifies → worker corrects → worker remains liable
The breach mechanism is:
AI output → apparent efficiency → hidden verification burden → staff stress → record risk → disciplinary / clinical / tribunal exposure
Core line:
AI does not remove work if the worker must verify the machine under threat.
Evidence Supported
NHS England announced that more than 500,000 NHS staff would receive Microsoft 365 Copilot following a trial of more than 30,000 workers across 90 NHS organisations, with an average claimed saving of 43 minutes per staff member per day. (NHS England)
NHS England also announced support for ambient voice technologies that capture clinician–patient conversations and use AI to generate real-time transcriptions and clinical summaries, with claimed savings of two to three minutes per consultation. (NHS England)
NHS Digital describes AI-enabled ambient scribes as tools that listen in the background to capture speech or conversations and produce task-specific outputs, such as summaries or letters. (NHS England Digital)
NHS England’s guidance describes ambient scribing products as generative-AI products used for clinical or patient documentation and workflow support. (NHS England)
The Health and Safety Executive identifies work-related stress risk through six work-design areas: demands, control, support, relationships, role, and change. (HSE)
Research on AI-generated clinical notes confirms that clinicians edit AI draft notes into final documentation and that the draft-to-final process varies by clinician, proving that AI note production is not a passive or complete substitution for professional review. (arXiv)
Together, those sources support the breach position:
AI productivity claims must be assessed against the verification, correction, supervision, liability, and stress burden placed on workers.
Mechanism Identified
The mechanism is:
AI produces output → output appears complete → worker must check output → worker must correct output → worker may become accountable for final use
This applies across:
- Copilot-generated summaries;
- drafted emails;
- meeting notes;
- policy summaries;
- patient-adjacent correspondence;
- ambient voice transcripts;
- AI-generated clinical summaries;
- triage outputs;
- referral drafts;
- complaint responses;
- staff audit records;
- and patient-record entries.
The risk arises because AI output can look coherent even where it is:
- incomplete;
- wrong;
- overconfident;
- hallucinated;
- clinically unsafe;
- missing context;
- missing negation;
- misreading tone;
- misreading urgency;
- omitting uncertainty;
- converting patient language into wrong clinical terminology;
- or inserting assumptions not present in the source material.
The worker then becomes the safety filter.
That is the burden transfer.
Legal Frameworks Engaged
This breach engages, at minimum:
- Health and Safety at Work etc. Act 1974 section 2 — safe system of work.
- Management of Health and Safety at Work Regulations 1999 — risk assessment.
- HSE Management Standards — demands, control, support, relationships, role, and change.
- Employer common law duty of care.
- Common law implied duty of mutual trust and confidence.
- Employment Rights Act 1996 section 98 — fairness in dismissal.
- Employment Rights Act 1996 section 47B — detriment for protected disclosure.
- Employment Rights Act 1996 section 103A — automatic unfair dismissal for protected disclosure.
- Public Interest Disclosure Act 1998.
- ACAS Code of Practice on Disciplinary and Grievance Procedures.
- Equality Act 2010 sections 19, 20–21 and 39 — indirect discrimination, reasonable adjustments, employment protections.
- Equality Act 2010 section 149 — Public Sector Equality Duty.
- Human Rights Act 1998 / ECHR Article 8 — private life, dignity, reputation, psychological integrity.
- Human Rights Act 1998 / ECHR Article 6 — fair process where AI outputs or logs are relied upon.
- Natural justice — right to know and answer the case.
- Employment Tribunal Rules / overriding objective — fair handling of AI-related evidence.
- UK GDPR Article 5(1)(a) — fairness and transparency.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 13 — staff-facing transparency where data is collected.
- UK GDPR Article 15 — access to AI-use records.
- UK GDPR Article 16 — rectification of inaccurate data.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 32 — security of processing.
- UK GDPR Article 35 — DPIA.
- Common Law Duty of Confidentiality where patient data is involved.
- Caldicott Principles.
- NHS Constitution — safe care, confidentiality, dignity, staff responsibilities and patient rights.
- NHS Records Management Code of Practice.
- DCB0129 / DCB0160 clinical safety standards where AI output affects clinical documentation or pathways.
- DTAC — clinical safety, data protection, technical security, interoperability, usability and accessibility.
- EU AI Act Article 9 — risk management.
- EU AI Act Article 10 — data governance.
- EU AI Act Article 11 — technical documentation.
- EU AI Act Article 12 — logs and record keeping.
- EU AI Act Article 13 — transparency and information to users.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness and cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- UN Guiding Principles on Business and Human Rights — prevention of adverse human-rights impacts through organisational systems.
Legal Duty
NHS England, NHS trusts, ICBs, GP practices, vendors, processors, and deploying organisations must ensure that AI systems do not shift unmanaged verification, correction, and liability burdens onto staff.
That duty includes assessing:
- what outputs AI creates;
- whether outputs are clinical, administrative, legal, disciplinary, or patient-record relevant;
- what human review is required;
- how long proper review takes;
- what error types are foreseeable;
- what hallucination safeguards exist;
- whether staff can identify hallucinations;
- whether verification time has been built into workload;
- whether staff are trained to reject AI output;
- whether staff are protected when AI output is wrong;
- whether audit trails distinguish AI error from staff error;
- and whether productivity claims account for verification time.
A time-saving claim is not valid unless it includes the time required to verify, correct, document, and safely rely on the output.
Breach Identified
The breach identified is the risk that NHS AI tools are presented as administrative relief while the actual legal and clinical burden is transferred to the worker.
The public narrative is:
AI saves time.
The operational reality may be:
AI generates work that must be checked.
That checking may include:
- verifying factual accuracy;
- checking clinical terminology;
- confirming patient details;
- checking confidentiality;
- checking data minimisation;
- checking hallucinated content;
- confirming source documents;
- correcting summaries;
- removing unsafe assumptions;
- checking legal wording;
- confirming patient consent;
- and ensuring final record integrity.
If the worker misses the error, the worker may be blamed.
That is a workforce-liability breach.
Hallucination and Output-Reliance Risk
AI hallucination does not need to be dramatic to be dangerous.
In healthcare, small errors can matter.
Examples include:
- adding a symptom not reported;
- omitting a symptom that was reported;
- changing “possible” into “confirmed”;
- changing “denies chest pain” into “chest pain”;
- omitting allergy information;
- confusing medication names;
- summarising mental health disclosures incorrectly;
- creating a confident letter from uncertain information;
- smoothing over safeguarding concern;
- or drafting correspondence that appears authoritative but lacks evidential basis.
The more polished the AI output, the greater the risk that the worker trusts it too quickly.
That creates a foreseeable safety and liability issue.
Verification Burden Risk
The verification burden is not neutral.
It is work.
It requires:
- time;
- concentration;
- context;
- training;
- source access;
- patient knowledge;
- policy knowledge;
- data-protection knowledge;
- clinical judgment where relevant;
- and confidence to reject the machine.
If management claims time savings while staff must verify every output, the employer must show the net effect.
The relevant calculation is not:
AI generation time saved
The relevant calculation is:
manual task time avoided minus verification time minus correction time minus incident time minus stress cost minus litigation risk
Without that calculation, the productivity claim is incomplete.
Workforce Stress Risk
The stress risk is foreseeable because AI changes the work environment across the HSE stress domains:
- demands — staff may be expected to process more because AI is said to save time;
- control — staff may have limited control over tools they are required to use;
- support — staff may lack training or specialist support;
- relationships — disputes may arise over whether an error was human or AI-created;
- role — staff may not know whether they are user, verifier, editor, data controller, or liability endpoint;
- change — mass deployment changes working practice rapidly. (HSE)
This links directly to Breach I, because public warning language about dismissal or prison intensifies the risk where the AI environment is not clearly governed.
Clinical Record Risk
Where AI output enters the clinical record, the risk becomes sharper.
The chain is:
AI draft → clinician verifies under pressure → error missed → record entered → future care relies on record → patient harm or complaint
The clinician may then be judged as if the AI error was their own professional failure.
That is not safe unless the system distinguishes:
- AI draft;
- human edits;
- final signed version;
- source material;
- correction history;
- and known AI limitations.
Staff Liability Risk
The staff liability chain is:
AI produces output → staff accepts or edits output → output later found wrong → employer investigates → audit trail attributes final action to worker → upstream model / vendor / deployment design becomes invisible
This is liability displacement.
The system makes the worker the visible endpoint.
But the error may have originated in:
- model design;
- poor training data;
- faulty retrieval;
- inadequate prompt design;
- transcription error;
- missing context;
- weak policy;
- poor training;
- workload pressure;
- or unsafe rollout.
Tribunal / Procedural Risk
This breach has direct tribunal relevance because AI outputs may be relied upon in:
- disciplinary proceedings;
- unfair dismissal claims;
- protected-disclosure detriment claims;
- whistleblowing dismissal claims;
- disability or equality claims;
- capability proceedings;
- professional-regulation referrals;
- negligence claims;
- data-protection complaints;
- and credibility disputes.
Where AI output is relied upon, the evidence chain must show:
- whether the content was AI-generated;
- what source material was used;
- what prompt or instruction produced it;
- what model version was used;
- what retrieval source was used;
- whether the output was checked;
- who checked it;
- what edits were made;
- what errors were known;
- what training the worker had;
- and whether workload made proper verification realistic.
Without that, the AI output is procedurally unsafe.
Disclosure Questions
- What AI outputs are NHS staff expected to verify?
- What outputs may enter clinical records?
- What outputs may enter patient correspondence?
- What outputs may enter complaints, HR, disciplinary, or tribunal material?
- What hallucination testing has been completed?
- What known error types have been documented?
- Are staff trained to detect hallucinations?
- Are staff trained to reject AI outputs?
- Are staff protected where AI output is wrong?
- Are staff given time to verify outputs?
- Is verification time included in the 43-minute saving claim?
- Is correction time included in the 43-minute saving claim?
- Is incident-review time included in productivity calculations?
- Is stress risk included in deployment assessments?
- Has an HSE-style stress risk assessment been completed?
- Has role ambiguity been assessed?
- Has workload increase from AI verification been assessed?
- Has equality impact on disabled, neurodivergent, older, lower-band, agency, or digitally less confident staff been assessed?
- Are AI drafts labelled as AI drafts?
- Are AI-generated outputs retained separately from final human-approved outputs?
- Is the source material retained?
- Is the prompt retained?
- Is the model version retained?
- Is edit history retained?
- Are hallucinated outputs recorded as incidents?
- Are near misses recorded?
- Can staff challenge audit attribution where error originated upstream?
- Can staff make protected disclosures about unsafe AI output?
- What disciplinary safeguards exist where AI error is involved?
- Who is liable where AI output is wrong but the staff member was under pressure to rely on it?
Evidence Relied Upon
EX-B14-01 — NHS England announcement of Microsoft 365 Copilot rollout to more than 500,000 staff after a trial of more than 30,000 workers across 90 NHS organisations and a claimed average saving of 43 minutes per staff member per day. (NHS England)
EX-B14-02 — NHS England announcement supporting ambient voice technologies that capture clinician–patient conversations and use AI to generate real-time transcriptions and clinical summaries. (NHS England)
EX-B14-03 — NHS Digital guidance describing AI-enabled ambient scribes as tools that listen in the background and produce task-specific outputs such as summaries or letters. (NHS England Digital)
EX-B14-04 — NHS England guidance describing ambient scribing products as generative-AI tools used for clinical or patient documentation and workflow support. (NHS England)
EX-B14-05 — HSE work-related stress guidance identifying demands, control, support, relationships, role, and change as key work-design areas affecting stress. (HSE)
EX-B14-06 — Research showing that ambient AI draft clinical notes are edited by clinicians into final documentation and that draft-to-final transformation varies by clinician. (arXiv)
Final Breach Position
This breach records that NHS AI deployment cannot rely on time-saving claims while ignoring the verification burden imposed on staff.
AI-generated output is not automatically safe output.
Where staff must check, correct, approve, sign, insert, send, or rely on AI content, that verification burden must be recognised as work, risk, stress, and potential liability.
Core line:
AI output is not free labour if a worker must carry the risk of making it safe.
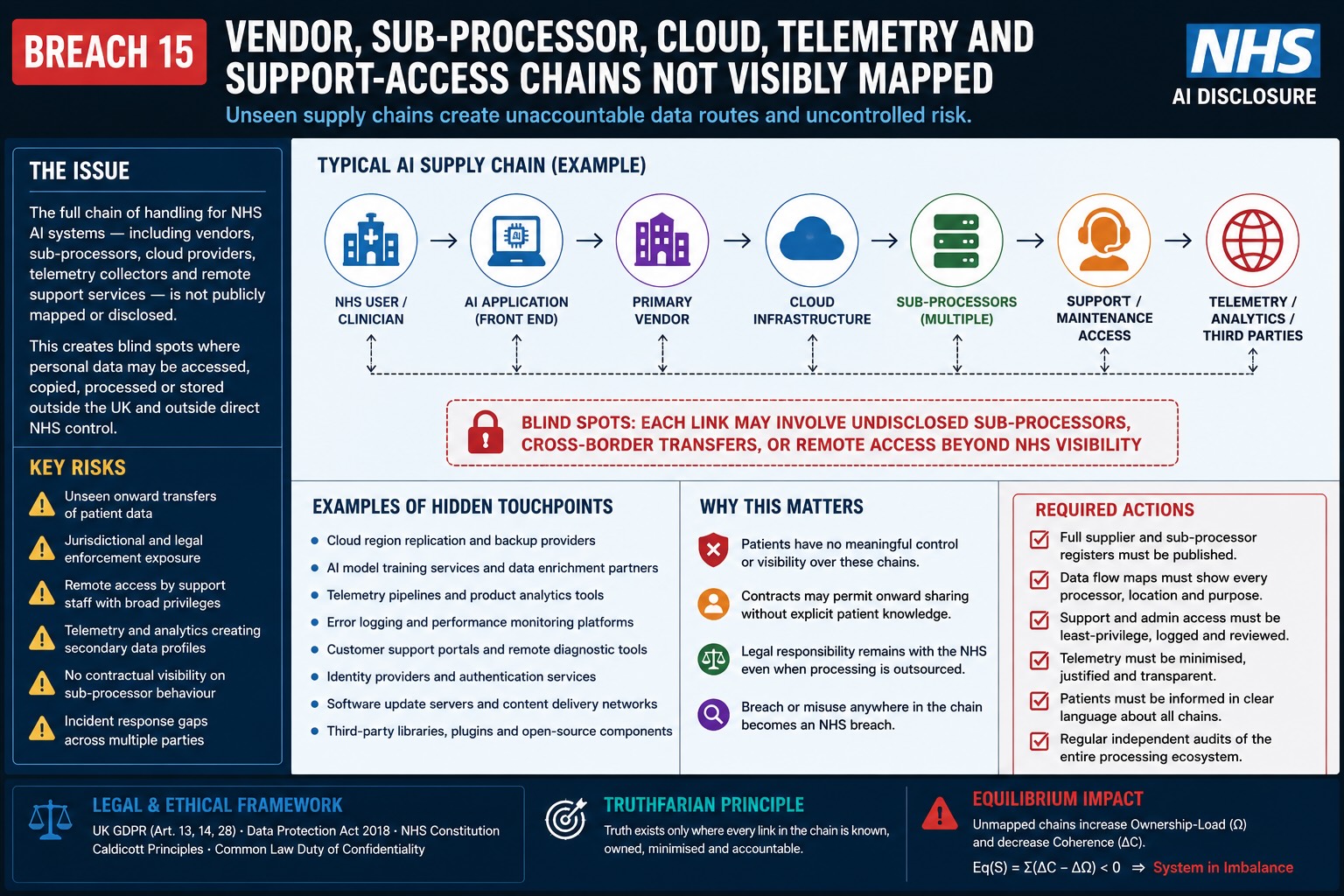
Breach 15 — Vendor, Sub-Processor, Cloud, Telemetry, and Support-Access Disclosure Failure. This figure shows how NHS AI processing can extend through vendors, sub-processors, cloud infrastructure, support access, telemetry, analytics, APIs, backup systems, and third-party services before the full handling chain is publicly mapped. The breach is the failure to disclose every processor, location, access route, logging pathway, onward transfer, and support mechanism that may touch patient or staff data, leaving hidden exposure points outside direct public visibility and control.
Breach XV — Vendor, Sub-Processor, Cloud, Telemetry, and Support-Access Disclosure Failure
Summary
This breach concerns the failure to visibly disclose the full vendor, processor, sub-processor, cloud, telemetry, support-access, model-service, analytics, and operational-processing chain behind NHS AI deployment.
The breach is not answered by naming the front-end product.
A patient or worker may see:
- NHS App;
- GP practice system;
- ambient scribe;
- AI triage tool;
- Microsoft Copilot;
- clinical workflow platform;
- or SaaS portal.
But the legal processing chain may include many more actors:
- controller;
- joint controller;
- processor;
- sub-processor;
- cloud host;
- AI model provider;
- speech-to-text provider;
- telemetry provider;
- security monitoring provider;
- analytics provider;
- support desk;
- disaster recovery provider;
- backup provider;
- product-improvement team;
- and cross-border operational support.
The breach mechanism is:
patient / worker data → NHS-facing system → vendor → cloud provider → AI service → logs → telemetry → support → sub-processors → undisclosed access / processing chain
Core line:
The public cannot assess sovereignty if the processing chain is hidden behind the product name.
Evidence Supported
NHS AI deployment involves multiple technology layers: AI triage, NHS App routing, ambient voice, AI scribing, Microsoft Copilot, cloud services, GP system integration, clinical documentation, patient-access tools, analytics, logs, and staff-facing workflow systems.
The issue is that public-facing material often identifies the visible product or the NHS body promoting deployment, but does not always visibly disclose the complete operational chain behind the system.
That chain matters because healthcare AI is not a single box.
It may involve:
- SaaS application layer;
- database layer;
- cloud compute layer;
- AI inference layer;
- speech-processing layer;
- security layer;
- logging layer;
- telemetry layer;
- analytics layer;
- support layer;
- and vendor governance layer.
Where the system processes health data, patient speech, staff prompts, clinical notes, triage answers, or audit logs, every layer may create legal consequences.
The evidence position is therefore:
NHS AI deployment cannot be assessed only at the user interface. It must be assessed across the full processor and sub-processor chain.
Mechanism Identified
The mechanism is:
front-end system → hidden operational chain → secondary processing → patient / staff rights risk
1. Front-end system
The patient or staff member interacts with a visible NHS or NHS-approved route.
Examples:
- NHS App;
- GP online triage;
- ambient scribe;
- Copilot-enabled workplace system;
- patient-access portal;
- voice transcription tool;
- appointment-booking tool.
2. Vendor processing
The product vendor may receive or process:
- patient data;
- staff data;
- symptom text;
- appointment request;
- voice data;
- transcript;
- generated summary;
- prompt;
- output;
- metadata;
- audit trail.
3. Cloud processing
Cloud infrastructure may provide:
- hosting;
- storage;
- compute;
- inference;
- backup;
- disaster recovery;
- monitoring;
- access control;
- encryption;
- logging.
4. AI service processing
The AI layer may provide:
- speech-to-text;
- summarisation;
- classification;
- triage reasoning;
- document retrieval;
- prompt processing;
- generated output;
- model monitoring.
5. Telemetry and analytics
The system may produce:
- performance metrics;
- latency data;
- error traces;
- usage data;
- staff activity data;
- patient pathway data;
- model confidence data;
- red-flag classification data;
- override data.
6. Support access
Support teams may access:
- logs;
- screenshots;
- tickets;
- diagnostic traces;
- user records;
- configuration data
- error reports;
- operational metadata.
This full chain must be disclosed.
Legal Frameworks Engaged
This breach engages, at minimum:
- UK GDPR Article 5(1)(a) — lawfulness, fairness, transparency.
- UK GDPR Article 5(1)(b) — purpose limitation.
- UK GDPR Article 5(1)(c) — data minimisation.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(e) — storage limitation.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 6 — lawful basis.
- UK GDPR Article 9 — special-category health data.
- UK GDPR Article 13 — information where data is collected directly.
- UK GDPR Article 14 — information where data is generated or obtained indirectly.
- UK GDPR Article 15 — right of access.
- UK GDPR Article 16 — rectification.
- UK GDPR Article 18 — restriction of processing.
- UK GDPR Article 21 — right to object.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 28 — processor and sub-processor obligations.
- UK GDPR Article 30 — records of processing activities.
- UK GDPR Article 32 — security of processing.
- UK GDPR Article 35 — Data Protection Impact Assessment.
- UK GDPR Articles 44–49 — international transfer safeguards.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality.
- Caldicott Principles.
- NHS Constitution — privacy, confidentiality, dignity, informed involvement, safe care.
- NHS Records Management Code of Practice.
- Human Rights Act 1998 / ECHR Article 8 — private life, medical privacy, dignity, bodily autonomy.
- Human Rights Act 1998 / ECHR Article 14 — non-discrimination.
- Public law rationality, proportionality and transparency.
- DCB0129 / DCB0160 clinical safety standards where vendor software affects clinical pathways or records.
- DTAC — clinical safety, data protection, technical security, interoperability, usability and accessibility.
- Algorithmic Transparency Recording Standard.
- EU AI Act Article 9 — risk management.
- EU AI Act Article 10 — data governance.
- EU AI Act Article 11 — technical documentation.
- EU AI Act Article 12 — record keeping / logs.
- EU AI Act Article 13 — transparency and provision of information.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness, cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- EU AI Act Article 50 — AI interaction / generated-output transparency where applicable.
- Convention 108+.
- OECD Privacy Guidelines.
- UNESCO Bioethics Article 9 — privacy and confidentiality.
- ICCPR Article 17 — privacy protection.
- UN Guiding Principles on Business and Human Rights.
Legal Duty
NHS England, ICBs, GP practices, NHS trusts, vendors, processors, and sub-processors must disclose and govern the full processing chain where patient or worker data is handled.
That duty includes identifying:
- controller;
- joint controllers if any;
- processor;
- sub-processors;
- cloud provider;
- AI model provider;
- speech-processing provider;
- analytics provider;
- telemetry provider;
- support provider;
- backup provider;
- disaster recovery provider;
- security monitoring provider;
- data centre region;
- execution region;
- support-access region;
- and transfer safeguards.
The duty is not satisfied by naming the NHS-facing product.
The legal duty follows the data.
Breach Identified
The breach identified is the apparent absence of a complete public-facing processor and sub-processor disclosure map for NHS AI deployment.
The public may be told:
- the system is NHS-approved;
- the system is integrated with NHS services;
- data is stored in the UK;
- or the system supports staff and patients.
But that does not disclose:
- who processes the data;
- who can access logs;
- who can access telemetry;
- who handles support tickets;
- who performs inference;
- who provides the model;
- who provides speech-to-text;
- who performs analytics;
- who monitors performance;
- who maintains backups;
- who has administrator access;
- and which legal jurisdictions apply.
That is the breach.
Sub-Processor Risk
Sub-processors matter because they may process the most legally sensitive data without being visible to the patient or worker.
A patient may think they are dealing with the NHS.
In reality, their data pathway may include:
NHS body → GP practice → SaaS vendor → cloud provider → AI model provider → telemetry provider → support provider
Each actor may create:
- access risk;
- transfer risk;
- purpose-change risk;
- retention risk;
- audit risk;
- re-identification risk;
- model-improvement risk;
- support-access risk.
The patient cannot meaningfully consent, object, or challenge processing if the chain is hidden.
Telemetry Risk
Telemetry is often treated as technical exhaust.
In healthcare AI, telemetry may carry clinical meaning.
Telemetry may reveal:
- what symptoms were entered;
- what question path was followed;
- what red flags were triggered;
- what urgency classification occurred;
- what output was generated;
- which clinician overrode the output;
- how long staff spent reviewing;
- what error occurred;
- what model failed;
- what patient group was affected.
That means telemetry may be personal data, health data, staff data, or evidential data.
It cannot be dismissed as neutral system data.
Support-Access Risk
Support access is a major blind spot.
Vendor support teams may need to troubleshoot:
- failed triage requests;
- incorrect outputs;
- transcription errors;
- integration failures;
- missing notes;
- user-access problems;
- audit-log problems;
- system crashes;
- and clinical workflow errors.
To resolve those issues, support may access operational records, screenshots, logs, transcripts, request data, or metadata.
That creates a lawful-access question:
Who can see what, from where, under what authority, for how long, and with what audit trail?
Sovereignty Risk
Sovereignty is not only about where the clinical database sits.
Sovereignty requires control over:
- compute;
- inference;
- logs;
- telemetry;
- support;
- backups;
- analytics;
- sub-processors;
- model services;
- operational access;
- transfer mechanisms;
- and exit capability.
A system may be UK-hosted and still be non-sovereign if key processing, support, model control, or operational dependency sits elsewhere.
Core line:
UK hosting does not equal UK control.
Staff and Tribunal Risk
This breach also creates employment and tribunal risk.
If AI prompts, outputs, logs, telemetry, support records, or audit trails are relied upon in disciplinary or tribunal proceedings, the worker must know:
- which system generated the record;
- which vendor processed it;
- whether sub-processors handled it;
- whether support accessed it;
- whether logs were complete;
- whether telemetry was interpreted correctly;
- whether foreign access occurred;
- whether model output was involved;
- and whether the record can be challenged.
A worker cannot fairly answer an allegation based on an opaque vendor chain.
Disclosure Questions
- What vendors are involved in NHS AI triage?
- What vendors are involved in ambient voice / AI scribing?
- What vendors are involved in Copilot-style staff AI tools?
- What cloud providers are used?
- What AI model providers are used?
- What speech-to-text providers are used?
- What analytics providers are used?
- What telemetry providers are used?
- What support providers are used?
- What backup providers are used?
- What disaster recovery providers are used?
- What security monitoring providers are used?
- What sub-processors process patient data?
- What sub-processors process staff data?
- What sub-processors process logs?
- What sub-processors process telemetry?
- What sub-processors process support tickets?
- What sub-processors process model-monitoring data?
- Where does inference occur?
- Where does speech-to-text occur?
- Where does summarisation occur?
- Where does support access occur?
- Where are logs stored and processed?
- Where is telemetry stored and processed?
- Are vendors permitted to use data for product improvement?
- Are vendors permitted to use data for model improvement?
- Are support screenshots allowed?
- Are support tickets redacted?
- Are sub-processors listed publicly?
- What public document maps the full chain from patient input to final output?
Evidence Relied Upon
EX-B15-01 — NHS AI triage materials showing patient symptom data is processed through AI / automated access pathways.
EX-B15-02 — NHS ambient voice and AI scribing materials showing consultation speech may be captured, transcribed, summarised, and inserted into clinical workflow.
EX-B15-03 — NHS Copilot deployment materials showing mass staff-facing AI deployment across NHS organisations.
EX-B15-04 — NHS data-protection and information-governance materials recognising processor, access-control, confidentiality, security, and special-category data obligations.
EX-B15-05 — Cloud / SaaS materials showing NHS digital environments rely on external vendors, infrastructure providers, and operational service providers.
EX-B15-06 — UK GDPR Article 28 processor obligation requiring processor and sub-processor governance.
EX-B15-07 — UK GDPR Article 30 records-of-processing obligation requiring processing activities to be recorded.
EX-B15-08 — UK GDPR Article 32 security-of-processing duty requiring appropriate technical and organisational measures.
Final Breach Position
This breach records that NHS AI deployment cannot be lawfully assessed by naming only the front-end product or stating that data is stored in the UK.
The full vendor, processor, sub-processor, cloud, AI-service, telemetry, support, analytics, backup, and operational-access chain must be disclosed.
Until that chain is visible, patients and staff cannot know who processes their data, where it acts, who may access it, how long it is retained, whether it is used for improvement, or what jurisdictional risks exist.
Core line:
The legal processor is not only the product patients see. It is the whole chain their data passes through.
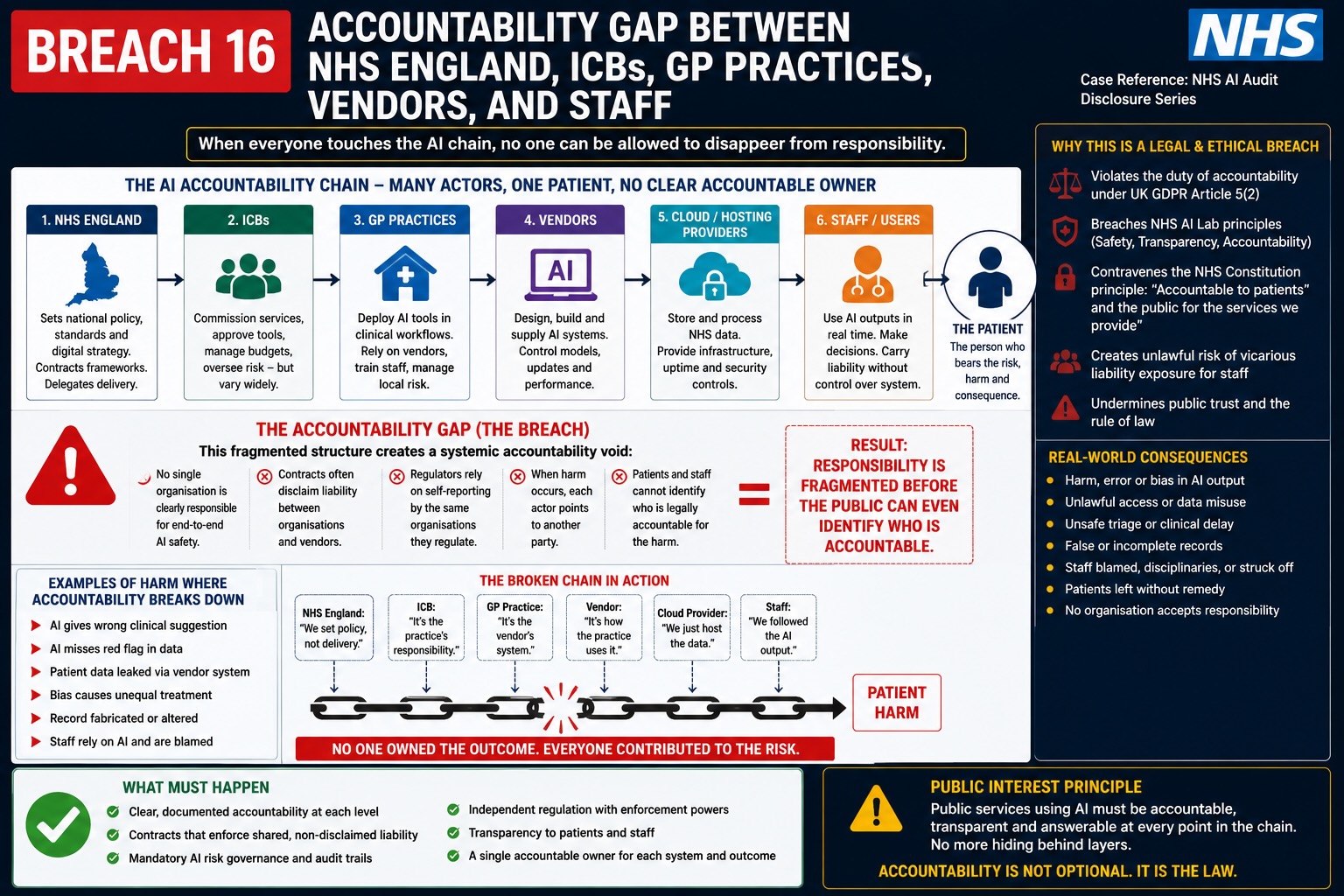
Breach 16 — Accountability Gap Between NHS England, ICBs, GP Practices, Vendors, and Staff. This figure shows how responsibility for NHS AI systems can become fragmented across national bodies, ICBs, GP practices, vendors, cloud providers, support teams, and frontline staff. The breach is the deployment of AI-mediated healthcare systems before the public record shows who is accountable for procurement, configuration, data processing, model output, clinical safety, audit trails, staff training, patient harm, vendor failure, and correction when something goes wrong.
Breach XVI — Accountability Gap Between NHS England, ICBs, GP Practices, Vendors, and Staff
Summary
This breach concerns the accountability gap created when NHS AI systems are deployed through a fragmented chain of national policy, local implementation, GP-practice adoption, vendor processing, cloud infrastructure, AI model operation, staff use, and patient-facing output.
The breach is not that multiple organisations are involved.
The breach is that accountability may become divided at the exact point where the patient or worker needs a single answer.
The patient may experience the system as “the NHS”.
The worker may experience the system as “an NHS-approved tool”.
But the legal chain may include:
- NHS England;
- ICBs;
- GP practices;
- NHS trusts;
- technology vendors;
- AI model providers;
- cloud providers;
- sub-processors;
- support teams;
- local system administrators;
- clinicians;
- reception staff;
- and information-governance teams.
The breach mechanism is:
national AI rollout → local deployment → vendor execution → staff operation → patient consequence → accountability dispersed
Core line:
A patient cannot be bounced between organisations when the AI system acts as one pathway.
Evidence Supported
NHS AI deployment is not a single institutional act.
It operates through a layered public-sector and vendor chain.
For example:
- NHS England may announce or accelerate national rollout;
- an ICB may support local adoption;
- a GP practice may deploy the tool;
- a vendor may provide the AI triage or ambient scribing system;
- a cloud provider may host or execute parts of the system;
- a model provider may perform inference, transcription, summarisation, or classification;
- staff may operate or verify outputs;
- and the patient may experience the final route, note, appointment, delay, correction, or refusal.
That creates a central governance question:
Who is legally accountable for the output?
Not generally.
Specifically.
For each AI-mediated event:
who owns the decision, who owns the data, who owns the error, who owns the audit trail, who owns the correction, and who owns the harm?
Mechanism Identified
The accountability gap arises because different actors may control different parts of the system.
1. NHS England
NHS England may set national strategy, approve national direction, issue guidance, announce rollout, support adoption, or create the public policy environment.
2. ICBs
ICBs may coordinate regional adoption, funding, governance, local assurance, procurement routes, digital strategy, and implementation.
3. GP practices / NHS providers
GP practices, trusts, and provider organisations may act as local deployers, controllers, clinical users, patient-facing service points, and operational decision-makers.
4. Vendors
Vendors may design, configure, process, support, update, monitor, and maintain the AI system.
5. Cloud / AI model providers
Cloud and model providers may execute compute, inference, speech-to-text, summarisation, logging, telemetry, analytics, backup, disaster recovery, or support functions.
6. Staff
Staff may become the visible human endpoint by approving, checking, correcting, overriding, or relying on AI output.
7. Patient
The patient suffers the consequence where access is delayed, redirected, misclassified, inaccurately recorded, or processed without meaningful consent.
The breach occurs where the system behaves as one pathway but accountability is split into fragments.
Legal Frameworks Engaged
This breach engages, at minimum:
- UK GDPR Article 5(1)(a) — lawfulness, fairness, transparency.
- UK GDPR Article 5(1)(b) — purpose limitation.
- UK GDPR Article 5(1)(c) — data minimisation.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 5(2) — accountability.
- UK GDPR Article 6 — lawful basis.
- UK GDPR Article 9 — special-category health data.
- UK GDPR Article 13 — transparency where data is collected directly.
- UK GDPR Article 14 — transparency where data is generated or obtained indirectly.
- UK GDPR Article 15 — right of access.
- UK GDPR Article 16 — rectification.
- UK GDPR Article 18 — restriction of processing.
- UK GDPR Article 21 — objection.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 24 — responsibility of the controller.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 26 — joint controllers where applicable.
- UK GDPR Article 28 — processor and sub-processor obligations.
- UK GDPR Article 30 — records of processing activities.
- UK GDPR Article 32 — security of processing.
- UK GDPR Article 35 — Data Protection Impact Assessment.
- UK GDPR Articles 44–49 — international transfer safeguards.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality.
- Caldicott Principles.
- NHS Constitution — privacy, confidentiality, safe care, informed involvement, complaints and redress.
- NHS Records Management Code of Practice.
- Human Rights Act 1998 / ECHR Article 8 — medical privacy, dignity, private life.
- Human Rights Act 1998 / ECHR Article 14 — non-discrimination.
- Equality Act 2010 sections 19, 20–21, 29 and 149.
- Common law negligence / duty of care.
- Duty of candour where AI-related harm or near-miss occurs.
- Public law rationality, proportionality, fairness and transparency.
- DCB0129 / DCB0160 clinical safety standards.
- DTAC.
- Algorithmic Transparency Recording Standard.
- Employment Rights Act 1996 sections 47B, 98 and 103A where staff liability or whistleblowing is engaged.
- Public Interest Disclosure Act 1998.
- ACAS Code of Practice where staff are disciplined using AI-related material.
- EU AI Act Article 9 — risk management.
- EU AI Act Article 10 — data governance.
- EU AI Act Article 11 — technical documentation.
- EU AI Act Article 12 — record keeping.
- EU AI Act Article 13 — transparency.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness, cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- Convention 108+.
- OECD Privacy Guidelines.
- UNESCO Bioethics Article 9 — privacy and confidentiality.
- ICCPR Article 17 — privacy protection.
- ICESCR Article 12 — right to health.
- UN Guiding Principles on Business and Human Rights.
Legal Duty
Each actor in the NHS AI chain must have a defined legal role.
The duty includes identifying:
- who is the controller;
- whether there are joint controllers;
- who is the processor;
- who are the sub-processors;
- who is the deployer;
- who is the system owner;
- who is the clinical safety owner;
- who owns the DPIA;
- who owns the Equality Impact Assessment;
- who owns the algorithmic transparency record;
- who owns the patient-facing notice;
- who owns the consent / objection pathway;
- who owns correction and rectification;
- who owns staff training;
- who owns incident reporting;
- who owns audit-log interpretation;
- who owns disciplinary-use boundaries;
- and who is liable where harm occurs.
Accountability must be mapped before deployment.
It cannot be reconstructed after harm.
Breach Identified
The breach identified is the apparent fragmentation of responsibility across NHS England, local NHS bodies, GP practices, vendors, cloud providers, AI model providers, and individual staff.
The public deployment pathway may present the system as a unified NHS service.
But when something goes wrong, accountability may fragment:
- NHS England may say local organisations deploy the system;
- ICBs may say GP practices are responsible;
- GP practices may say the vendor provides the tool;
- vendors may say clinicians define protocols;
- cloud providers may say they only provide infrastructure;
- staff may say they followed the system;
- and patients may be left without a clear responsible party.
That is the breach.
A healthcare AI pathway cannot be lawful if responsibility dissolves at the moment of challenge.
Patient Redress Risk
The patient-redress risk chain is:
patient uses AI route → wrong output produced → patient delayed or misdirected → patient asks who is responsible → organisations point to different parts of the chain
The patient may need to know:
- who made the triage decision;
- who configured the pathway;
- who approved the protocol;
- who processed the data;
- who retained the logs;
- who can correct the record;
- who can explain the output;
- who investigates the incident;
- who compensates harm;
- and who prevents recurrence.
If the answer is unclear, the system denies practical redress.
Staff Liability Risk
The staff-liability risk chain is:
AI system produces output → staff uses or verifies output → issue arises → employer attributes final responsibility to worker → upstream system design becomes invisible
That creates a structural unfairness.
The staff member may not control:
- procurement;
- model selection;
- system configuration;
- vendor contract;
- logging design;
- patient notice;
- DPIA;
- clinical safety case;
- training design;
- telemetry;
- support access;
- or algorithmic transparency.
Yet the worker may be treated as the accountable endpoint.
That connects directly to Breaches I, II, X and XIV.
Vendor Accountability Risk
The vendor may control the technical system but not hold the visible public duty of care.
That creates a split between:
technical control
and
public accountability
If the vendor controls model behaviour, software updates, triage logic, interface design, logs, telemetry, support access, and processing infrastructure, the vendor’s role must be visible.
Patients and staff cannot assess risk if the party controlling the technical behaviour is hidden behind NHS branding.
Controller / Processor Risk
The data-protection accountability risk is:
unclear controller identity → unclear lawful basis → unclear privacy notice → unclear rights route → unclear correction route → unclear liability
For each NHS AI use case, the public record must identify whether:
- NHS England is controller;
- the GP practice is controller;
- the trust is controller;
- the ICB is controller;
- the vendor is processor;
- the vendor is joint controller;
- the cloud provider is sub-processor;
- the model provider is sub-processor;
- or any actor determines purposes and means.
Where purposes and means are shared, joint-controller duties may arise.
Where processing is carried out on behalf of the controller, processor duties arise.
The public must not be left guessing.
Clinical Safety Accountability Risk
Clinical safety requires named responsibility.
For AI triage, ambient voice, AI scribing, and clinical documentation systems, the accountability questions include:
- who owns the hazard log;
- who is the clinical safety officer;
- who approved residual risk;
- who monitors incidents;
- who receives safety reports;
- who can suspend the system;
- who reviews under-triage;
- who reviews transcription errors;
- who reviews hallucinated notes;
- who informs patients;
- and who reports harm.
A system cannot be clinically safe if no one visible owns the safety case.
Tribunal / Procedural Risk
This breach has direct tribunal and procedural relevance.
Where AI-related material is relied upon in employment, whistleblowing, negligence, equality, data-protection, judicial-review, regulatory, or disciplinary proceedings, accountability must be traceable.
A tribunal or court may need to know:
- who generated the record;
- who controlled the system;
- who processed the data;
- who retained the log;
- who interpreted the output;
- who had access;
- who could correct the data;
- who trained the worker;
- who approved the policy;
- who accepted the risk;
- and who is responsible for the decision.
Without accountability mapping, AI-derived evidence is procedurally unsafe.
Disclosure Questions
- Who is the controller for AI triage data?
- Who is the controller for ambient voice data?
- Who is the controller for Copilot staff-use data?
- Who is the controller for AI logs and telemetry?
- Are any parties joint controllers?
- Who are the processors?
- Who are the sub-processors?
- Who is the AI deployer?
- Who is the system owner?
- Who owns the DPIA?
- Who owns the clinical safety case?
- Who owns the Equality Impact Assessment?
- Who owns the Algorithmic Transparency Record?
- Who owns patient-facing consent notices?
- Who owns the opt-out route?
- Who owns correction and rectification?
- Who owns incident investigation?
- Who owns under-triage review?
- Who owns ambient voice transcription error review?
- Who owns AI hallucination incident review?
- Who owns staff training?
- Who owns staff disciplinary-use boundaries?
- Who owns audit-log interpretation?
- Who decides whether AI output can be used as evidence?
- Who can suspend the AI system?
- Who compensates the patient where harm occurs?
- Who protects the worker where AI error is wrongly attributed to them?
- Who answers a subject access request for AI-generated data?
- Who answers a patient complaint about AI routing?
- What single public accountability map identifies all responsible actors?
Evidence Relied Upon
EX-B16-01 — NHS AI triage deployment materials showing national policy and patient-access AI routing.
EX-B16-02 — NHS ambient voice / AI scribing materials showing AI-mediated clinical documentation.
EX-B16-03 — NHS Copilot deployment materials showing mass staff-facing AI deployment.
EX-B16-04 — NHS information-governance materials recognising controller, processor, access-control, confidentiality, and data-protection duties.
EX-B16-05 — Vendor / SaaS / cloud material showing that NHS AI pathways may depend on external technical providers and operational support.
EX-B16-06 — UK GDPR Article 5(2) accountability principle.
EX-B16-07 — UK GDPR Article 24 controller responsibility.
EX-B16-08 — UK GDPR Article 26 joint-controller duty where purposes and means are jointly determined.
EX-B16-09 — UK GDPR Article 28 processor and sub-processor obligations.
Final Breach Position
This breach records that NHS AI deployment creates a serious accountability gap if national bodies, local deployers, GP practices, vendors, cloud providers, model providers, and staff all control different parts of the pathway but no single public accountability map exists.
Patients and workers must not be forced to trace responsibility through a hidden chain after harm occurs.
Where AI acts as one healthcare pathway, accountability must also be visible as one coherent chain.
Core line:
Fragmented deployment cannot be allowed to become fragmented responsibility.
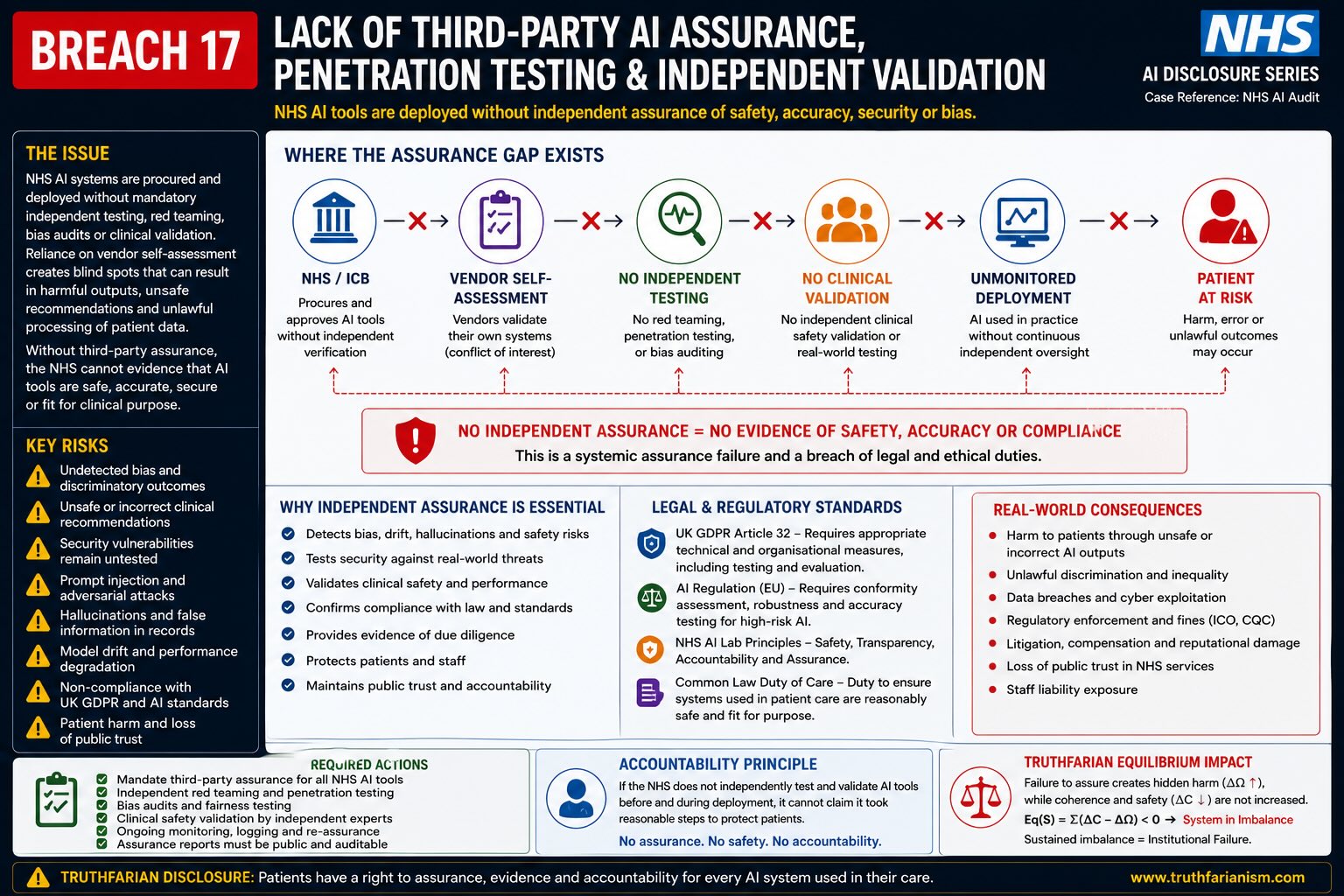
Breach 17 — Lack of Third-Party AI Assurance, Penetration Testing and Independent Validation. This figure illustrates the absence of mandatory independent assurance throughout the NHS AI procurement and deployment lifecycle. It shows how AI systems may progress from procurement and vendor self-assessment into clinical deployment without independent security testing, red teaming, penetration testing, bias assessment, clinical validation or continuous external oversight. The diagram highlights the resulting risks, including undetected model drift, hallucinations, discriminatory outcomes, security vulnerabilities, unlawful processing, patient harm and regulatory liability. It further identifies the legal and governance obligations requiring appropriate technical and organisational safeguards, demonstrating that reliance on vendor self-assessment alone does not provide objective evidence that AI systems are safe, accurate, secure or clinically fit for purpose before deployment within patient care.
Breach XVII — AI Output Reliance in Employment, Disciplinary, Tribunal, and Protected-Disclosure Contexts
Summary
This breach concerns the risk that AI-generated, AI-assisted, AI-mediated, or AI-logged material may later be relied upon in employment, disciplinary, tribunal, whistleblowing, regulatory, clinical, or procedural contexts before the AI evidence chain has been disclosed and tested.
The breach is not only that AI may be used in NHS work.
The breach is that AI output may later become evidence.
That evidence may include:
- prompts;
- AI-generated summaries;
- ambient voice transcripts;
- AI clinical notes;
- triage outputs;
- routing decisions;
- staff usage logs;
- audit trails;
- access records;
- telemetry;
- model-monitoring records;
- AI-drafted emails;
- AI-generated HR notes;
- AI-generated complaint responses;
- AI-assisted investigation records;
- and AI-linked disciplinary material.
The breach mechanism is:
AI system produces or records material → employer / NHS body / vendor retains it → material is later relied upon against patient or worker → affected person cannot test the AI chain
Core line:
AI output is not safe evidence unless its source, system, model, prompt, processing path, human review, and audit chain are disclosed.
Evidence Supported
This breach is supported by the preceding disclosure architecture.
The NHS AI environment now includes:
- mass staff-facing AI tools;
- patient-access AI triage;
- ambient voice technology;
- AI scribing;
- workflow summarisation;
- staff audit logs;
- patient-record access warnings;
- cloud and SaaS processing;
- vendor support;
- telemetry;
- and AI-generated clinical or administrative outputs.
That creates a foreseeable evidence pathway:
AI use today → record retained → dispute tomorrow → AI-derived material relied upon as fact
This matters because NHS staff may later face:
- disciplinary allegation;
- dismissal;
- professional referral;
- information-governance allegation;
- patient-record access allegation;
- capability allegation;
- misconduct allegation;
- protected-disclosure detriment;
- or tribunal proceedings.
Patients may also face AI-derived material in:
- complaints;
- negligence disputes;
- safeguarding disputes;
- data-protection disputes;
- access disputes;
- clinical-record correction disputes;
- and coronial or regulatory investigations.
The breach is therefore evidence integrity.
Mechanism Identified
The mechanism is:
AI-mediated event → retained record → institutional interpretation → procedural reliance
1. AI-mediated event
An event occurs inside an AI-enabled pathway.
Examples:
- staff member uses Copilot;
- patient uses AI triage;
- clinician uses ambient scribe;
- receptionist processes an AI-routed request;
- worker checks an AI-generated note;
- clinician overrides a triage output;
- AI generates a draft letter;
- and the system logs access or prompt activity.
2. Retained record
The system may retain:
- input;
- prompt;
- output;
- summary;
- transcript;
- timestamp;
- user ID;
- document reference;
- audit log;
- model version;
- telemetry;
- correction history;
- or support record.
3. Institutional interpretation
Later, the organisation may interpret the record as showing:
- misconduct;
- inappropriate access;
- failure to follow policy;
- clinical error;
- patient-contact failure;
- productivity issue;
- poor performance;
- failure to verify AI output;
- breach of confidentiality;
- or unreliable patient account.
4. Procedural reliance
The record may then be relied upon in:
- HR investigation;
- disciplinary meeting;
- grievance;
- whistleblowing detriment dispute;
- employment tribunal;
- professional-regulation referral;
- data-protection complaint;
- clinical negligence case;
- or judicial review.
This is where the breach crystallises.
Legal Frameworks Engaged
This breach engages, at minimum:
- Employment Rights Act 1996 section 47B — detriment for protected disclosure.
- Employment Rights Act 1996 section 98 — fairness in dismissal.
- Employment Rights Act 1996 section 103A — automatic unfair dismissal for protected disclosure.
- Public Interest Disclosure Act 1998.
- ACAS Code of Practice on Disciplinary and Grievance Procedures.
- Common law implied duty of mutual trust and confidence.
- Employer common law duty of care.
- Natural justice — right to know and answer the case.
- Employment Tribunal Rules / overriding objective — fair and just disposal.
- Human Rights Act 1998 / ECHR Article 6 — fair hearing.
- Human Rights Act 1998 / ECHR Article 8 — private life, reputation, dignity, psychological integrity.
- Equality Act 2010 sections 19, 20–21, 39 and 149 — indirect discrimination, reasonable adjustments, employment protections, Public Sector Equality Duty.
- UK GDPR Article 5(1)(a) — lawfulness, fairness, transparency.
- UK GDPR Article 5(1)(b) — purpose limitation.
- UK GDPR Article 5(1)(c) — data minimisation.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 5(2) — accountability.
- UK GDPR Article 6 — lawful basis.
- UK GDPR Article 9 — special-category health data where patient or health-worker data is involved.
- UK GDPR Article 13 — information where data is collected from the worker or patient.
- UK GDPR Article 14 — information where derived data is generated indirectly.
- UK GDPR Article 15 — right of access.
- UK GDPR Article 16 — rectification.
- UK GDPR Article 18 — restriction of processing.
- UK GDPR Article 21 — objection.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 28 — processor obligations.
- UK GDPR Article 30 — records of processing activities.
- UK GDPR Article 32 — security of processing.
- UK GDPR Article 35 — DPIA.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality where patient data is involved.
- Caldicott Principles.
- NHS Records Management Code of Practice.
- NHS Constitution — confidentiality, dignity, complaints, redress, safe care.
- DCB0129 / DCB0160 clinical safety standards where AI material affects clinical pathways or records.
- Algorithmic Transparency Recording Standard.
- EU AI Act Article 9 — risk management.
- EU AI Act Article 10 — data governance.
- EU AI Act Article 11 — technical documentation.
- EU AI Act Article 12 — record keeping / logs.
- EU AI Act Article 13 — transparency and provision of information.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness and cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- EU AI Act Article 50 — AI-generated output transparency where applicable.
- UN Guiding Principles on Business and Human Rights.
Legal Duty
NHS England, NHS bodies, employers, GP practices, vendors, processors, and tribunals relying on AI-derived material must ensure that AI evidence is disclosed, explainable, accurate, complete, and procedurally fair.
That duty includes identifying:
- whether the material was AI-generated, AI-assisted, or human-authored;
- what system created it;
- what model or engine was used;
- what prompt, input, or source material generated it;
- what version of the system was active;
- whether the output was edited;
- who edited it;
- what was accepted or rejected;
- whether the output was checked;
- whether logs are complete;
- whether timestamps are reliable;
- whether the record contains inference, not fact;
- whether the affected person can access it;
- whether the affected person can correct it;
- and whether the material is safe to rely upon.
AI evidence must not be treated as ordinary documentary evidence without disclosing its generation chain.
Breach Identified
The breach identified is the risk that AI-derived material becomes procedurally relied upon before the AI evidence chain is disclosed.
The ordinary paper trail is being replaced or supplemented by a machine-mediated trail.
That trail may look complete, but may contain:
- generated content;
- inferred content;
- hallucinated content;
- omitted context;
- inaccurate transcription;
- incomplete logs;
- hidden prompts;
- hidden telemetry;
- system-generated metadata;
- vendor-normalised records;
- and audit interpretations.
If an employer, NHS body, regulator, or tribunal relies on that material without disclosing the full AI chain, the affected person cannot answer the case.
That is the procedural breach.
Protected-Disclosure Risk
This breach is especially serious in protected-disclosure contexts.
A worker who raises concerns about AI safety, patient-data misuse, unsafe triage, ambient voice errors, unlawful processing, inadequate training, or misleading productivity claims may later face AI-derived records being used against them.
The risk chain is:
worker raises AI concern → employer reviews AI logs / emails / prompts / usage records → AI-derived material used to reframe worker conduct → detriment or dismissal follows
That creates a PIDA risk.
If AI-derived material is used after a protected disclosure, the employer must prove that reliance is fair, accurate, proportionate, and not retaliatory.
Where the AI chain is opaque, that proof is weakened.
Employment Disciplinary Risk
In disciplinary proceedings, AI material may be used to allege:
- inappropriate record access;
- patient-data misuse;
- breach of confidentiality;
- failure to follow AI policy;
- failure to verify output;
- poor performance;
- inaccurate record keeping;
- refusal to use AI;
- excessive use of AI;
- or unsafe use of AI.
Fair process requires the worker to receive:
- the raw record;
- the AI-generated record;
- the system log;
- the policy in force at the time;
- the training record;
- the model / system explanation;
- the audit interpretation;
- the human-review record;
- and the opportunity to challenge accuracy.
Without that, the disciplinary process is unsafe.
Tribunal Evidence Risk
Where AI-derived material is placed before a tribunal, the tribunal must know whether it is:
- primary evidence;
- generated evidence;
- summarised evidence;
- inferred evidence;
- reconstructed evidence;
- audit metadata;
- or opinion-like machine output.
The procedural issue is:
AI output can look like fact while functioning as interpretation.
A tribunal cannot assess weight, reliability, fairness, or admissibility unless the AI generation chain is disclosed.
Patient-Record Evidence Risk
AI-generated clinical notes, ambient voice summaries, triage outputs, and patient-access logs may later be used as evidence of what a patient said, what a clinician did, or what route was selected.
That creates risk where:
- the original audio is deleted;
- the transcript is not retained;
- the AI draft is overwritten;
- edit history is unavailable;
- prompts are not disclosed;
- model version is unknown;
- and the final record appears human-authored.
The patient may then be forced to challenge an official medical record without seeing the AI mediation that produced it.
That is procedurally unfair.
Data Accuracy and Rectification Risk
AI-derived records may contain inaccurate personal data.
Under data-protection principles, the affected person must be able to access and correct inaccurate data.
But AI records may exist across multiple layers:
- clinical record;
- draft note;
- transcript;
- prompt log;
- system log;
- vendor log;
- telemetry;
- support ticket;
- model-monitoring record;
- and audit extract.
If only the final record is corrected but the AI-derived underlying records remain wrong, the inaccuracy persists.
That creates continuing processing harm.
Tribunal / Procedural Disclosure Requirements
Where AI material is relied upon, disclosure should include:
- original input;
- prompt;
- source documents;
- AI output;
- draft versions;
- final version;
- edit history;
- user identity;
- timestamps;
- model / system version;
- vendor identity;
- processing location;
- log-retention policy;
- audit interpretation;
- human-review record;
- correction history;
- and training / policy documents in force at the time.
Without this, the affected person cannot test the reliability of the material.
Disclosure Questions
- Can AI-generated material be used in NHS disciplinary proceedings?
- Can AI prompts be used in disciplinary proceedings?
- Can AI outputs be used in tribunal proceedings?
- Can AI audit logs be used as evidence?
- Can ambient voice summaries be used as evidence of what was said?
- Can AI triage outputs be used as evidence of patient urgency?
- Can Copilot usage records be used in staff performance assessment?
- Are AI-generated documents labelled as AI-generated?
- Are AI-assisted documents labelled as AI-assisted?
- Are prompts retained?
- Are prompts disclosed to affected workers or patients?
- Are outputs retained?
- Are drafts retained?
- Are edit histories retained?
- Are model versions retained?
- Are source documents retained?
- Are raw audio files retained where ambient voice is used?
- Are transcripts retained?
- Are telemetry records retained?
- Are support records retained?
- Are staff told AI-use records may be used against them?
- Are patients told AI-generated notes may be relied upon later?
- Can workers correct inaccurate AI logs?
- Can patients correct inaccurate AI-generated notes?
- What policy governs AI material in disciplinary proceedings?
- What policy governs AI material in tribunal disclosure?
- What policy governs AI material in protected-disclosure cases?
- What safeguards prevent AI material being used retaliatorily after whistleblowing?
- What safeguards distinguish human error from AI system error?
- What evidence chain must be produced before AI material is relied upon?
Evidence Relied Upon
EX-B17-01 — NHS staff-facing AI deployment materials showing mass AI use may create named-user prompts, outputs, workflow records, and audit trails.
EX-B17-02 — NHS AI triage materials showing AI-generated patient-access outputs may be created and retained.
EX-B17-03 — NHS ambient voice / AI scribing materials showing AI-generated transcripts and clinical summaries may enter clinical documentation pathways.
EX-B17-04 — NHS patient-record access warning materials showing staff may face disciplinary or criminal consequences for improper data access.
EX-B17-05 — UK GDPR accuracy, access, rectification, transparency, and accountability duties.
EX-B17-06 — Employment Rights Act / PIDA protections where workers raise public-interest concerns.
EX-B17-07 — Article 6 ECHR / natural justice principles requiring fair opportunity to know and answer the case.
Final Breach Position
This breach records that NHS AI deployment creates a new evidential class: AI-derived material.
That material may appear factual, complete, and authoritative, while actually being generated, inferred, summarised, transformed, logged, or interpreted by a system whose chain is not visible.
Where such material is used in employment, disciplinary, tribunal, clinical, protected-disclosure, regulatory, or patient-record disputes, the AI chain must be disclosed before reliance.
Core line:
AI-generated material cannot become evidence while the machine that made it remains hidden.
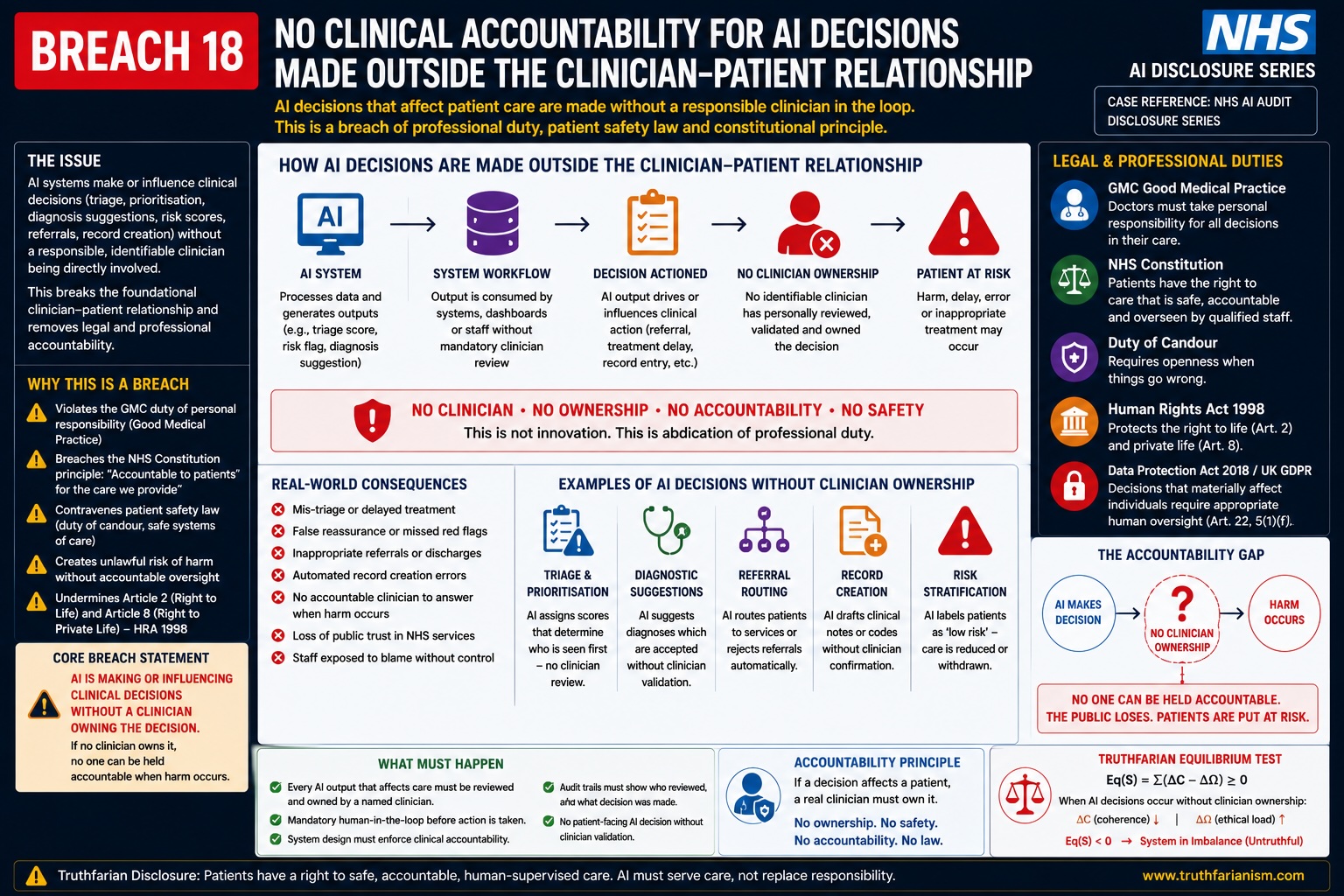
Breach 18 — No Clinical Accountability for AI Decisions Made Outside the Clinician-Patient Relationship. This figure shows how AI systems can make or influence clinical decisions through triage, prioritisation, diagnosis suggestions, risk scoring, referrals, record creation, or treatment-routing outputs without a clearly identifiable clinician owning the decision. The breach is the removal of accountable clinical judgment from the patient-care pathway, creating a gap where AI output may affect care while no responsible clinician has reviewed, validated, accepted, or answered for the decision before harm occurs.
Breach XVIII — Public-Sector AI Dependency, Foreign-Controlled Infrastructure, and Exit-Risk Failure
Summary
This breach concerns the creation of public-sector dependency on AI, SaaS, cloud, model, vendor, and proprietary infrastructure before the NHS has visibly disclosed a sovereign continuity and exit plan.
The breach is not merely that the NHS uses external technology.
The breach is that patient access, staff workflow, clinical documentation, triage routing, productivity claims, audit trails, and healthcare administration may become dependent on systems the NHS does not fully own, control, inspect, reproduce, or exit from without operational disruption.
The breach mechanism is:
national AI adoption → workflow dependency → proprietary vendor / cloud / model reliance → reduced public-sector control → exit difficulty → healthcare continuity risk
Core line:
A public health system cannot become operationally dependent on AI infrastructure it cannot independently control, audit, or replace.
Evidence Supported
NHS England states that more than 500,000 NHS staff are to receive Microsoft 365 Copilot after a trial involving over 30,000 workers across 90 NHS organisations, with claimed average savings of 43 minutes per staff member per day. (NHS England)
Microsoft describes the same NHS England Copilot adoption as intended to improve service delivery, reduce costs, and create more time for care. (Source)
NHS England also states that the NHS App’s new AI triage tool is being rolled out after a successful trial, with expected reach to over 200,000 patients within 12 months and availability to all NHS App users by April 2028. (NHS England)
NHS England’s ambient scribing guidance states that ambient scribing products feature generative AI and include advanced ambient voice technologies used for clinical or patient documentation and workflow support. (NHS England)
NHS Digital’s information-governance guidance confirms that NHS guidance now addresses AI-enabled ambient scribing products for patients, staff and IG professionals. (NHS England Digital)
Those facts support the dependency pathway:
staff productivity → patient access → clinical documentation → AI workflow → external platforms → operational reliance
The issue is not whether those products may be useful.
The issue is whether national healthcare operations become dependent before sovereignty, continuity, reversibility, portability, auditability, and fallback have been proven.
Mechanism Identified
The mechanism is:
AI system introduced → staff adapt workflow → patients are routed through it → records are generated through it → management measures productivity through it → organisation plans capacity around it → vendor/platform becomes structurally embedded
Dependency forms when the organisation begins to rely on the system for:
- staff productivity;
- patient triage;
- appointment routing;
- clinical summaries;
- meeting notes;
- correspondence;
- record formation;
- workflow prioritisation;
- administrative processing;
- audit trails;
- performance reporting;
- and cost-saving calculations.
Once that happens, the AI system stops being optional.
It becomes infrastructure.
That is the breach point.
Legal Frameworks Engaged
This breach engages, at minimum:
- UK GDPR Article 5(1)(a) — lawfulness, fairness, transparency.
- UK GDPR Article 5(1)(b) — purpose limitation.
- UK GDPR Article 5(1)(c) — data minimisation.
- UK GDPR Article 5(1)(d) — accuracy.
- UK GDPR Article 5(1)(f) — integrity and confidentiality.
- UK GDPR Article 5(2) — accountability.
- UK GDPR Article 6 — lawful basis.
- UK GDPR Article 9 — special-category health data.
- UK GDPR Article 13 — transparency.
- UK GDPR Article 14 — indirect / derived data transparency.
- UK GDPR Article 15 — access.
- UK GDPR Article 16 — rectification.
- UK GDPR Article 18 — restriction.
- UK GDPR Article 20 — portability where applicable.
- UK GDPR Article 21 — objection.
- UK GDPR Article 22 — automated decision-making / profiling where applicable.
- UK GDPR Article 24 — controller responsibility.
- UK GDPR Article 25 — data protection by design and default.
- UK GDPR Article 28 — processor and sub-processor governance.
- UK GDPR Article 30 — records of processing activities.
- UK GDPR Article 32 — security, resilience, availability and recovery.
- UK GDPR Article 35 — DPIA.
- UK GDPR Articles 44–49 — international transfer safeguards.
- Data Protection Act 2018.
- Common Law Duty of Confidentiality.
- Caldicott Principles.
- NHS Constitution — privacy, confidentiality, safe care, patient access, informed involvement.
- NHS Records Management Code of Practice.
- Human Rights Act 1998 / ECHR Article 8 — medical privacy, private life, dignity.
- Human Rights Act 1998 / ECHR Article 14 — non-discrimination.
- Equality Act 2010 sections 19, 20–21, 29 and 149.
- Common law negligence / duty of care.
- Duty of candour where dependency failure causes harm or near-miss.
- Public law rationality, proportionality and transparency.
- Public procurement transparency and value-for-money duties where applicable.
- Public-sector continuity / resilience duties where critical services are affected.
- DCB0129 / DCB0160 clinical safety standards where dependency affects clinical systems.
- DTAC technical security, interoperability, usability and accessibility requirements.
- Algorithmic Transparency Recording Standard.
- EU AI Act Article 9 — risk management.
- EU AI Act Article 10 — data governance.
- EU AI Act Article 11 — technical documentation.
- EU AI Act Article 12 — record keeping / logs.
- EU AI Act Article 13 — transparency.
- EU AI Act Article 14 — human oversight.
- EU AI Act Article 15 — accuracy, robustness and cybersecurity.
- EU AI Act Article 26 — deployer obligations where applicable.
- EU AI Act Article 50 — transparency where applicable.
- Convention 108+.
- OECD Privacy Guidelines.
- UNESCO Bioethics Article 5 — autonomy and individual responsibility.
- UNESCO Bioethics Article 6 — consent.
- UNESCO Bioethics Article 9 — privacy and confidentiality.
- UNESCO Bioethics Article 10 — equality, justice and equity.
- ICCPR Article 17 — privacy protection.
- ICESCR Article 12 — right to health.
- UN Guiding Principles on Business and Human Rights.
Legal Duty
NHS England and deploying NHS bodies must ensure that AI adoption does not create operational dependency without lawful continuity safeguards.
That duty includes proving:
- who controls the system;
- who controls the model;
- who controls the data;
- who controls the logs;
- who controls the audit trail;
- who controls system updates;
- who controls service suspension;
- who controls pricing changes;
- who controls contractual renewal;
- who controls support access;
- who controls export and migration;
- whether data can be returned in usable form;
- whether AI outputs can be audited after exit;
- whether workflows can continue without the vendor;
- whether equivalent human routes remain;
- whether an open or sovereign replacement exists;
- and whether critical healthcare operations can continue if service is withdrawn, restricted, degraded, repriced, or legally constrained.
A public health system must not place critical access, documentation, or workforce functions into an external dependency without a public exit architecture.
Breach Identified
The breach identified is the apparent absence of a visible sovereign exit and continuity plan for NHS AI deployment.
The public record shows acceleration.
It does not visibly show reversibility.
That matters because the NHS is not buying a simple office tool.
It is embedding AI into:
- patient front-door access;
- triage routing;
- clinical documentation;
- ambient voice capture;
- staff administration;
- productivity calculations;
- audit records;
- and operational performance.
If the NHS becomes dependent on a vendor system for those functions, then exit becomes difficult.
The legal question becomes:
Can the NHS continue safely if the vendor, model, platform, cloud provider, licence, contract, legal regime, price, or access condition changes?
If that cannot be answered, the dependency is unmanaged.
Foreign-Controlled Infrastructure Risk
Foreign-controlled infrastructure does not automatically mean unlawful processing.
But it creates sovereignty questions.
Those questions include:
- Can a foreign-controlled provider alter terms?
- Can access be suspended?
- Can pricing change after dependency forms?
- Can features be withdrawn?
- Can model behaviour change?
- Can support move jurisdiction?
- Can telemetry rules change?
- Can legal compulsion affect access or disclosure?
- Can the NHS independently audit the system?
- Can the NHS reproduce the service if the provider exits?
- Can the NHS migrate without losing audit continuity?
The issue is not hostility to foreign vendors.
The issue is public-sector dependency on infrastructure that may not be under public control.
Vendor Lock-In Risk
Vendor lock-in arises where:
- staff workflows are redesigned around one platform;
- documents are generated in proprietary formats;
- logs remain in vendor systems;
- AI summaries become part of records;
- prompts and outputs are not portable;
- integration is deep with clinical systems;
- training is platform-specific;
- dashboards rely on vendor analytics;
- audit histories are difficult to export;
- contracts renew under operational pressure;
- and replacement would disrupt care.
The more successful the AI rollout appears, the deeper the lock-in risk becomes.
That is why exit must be designed before adoption, not after dependency.
Clinical Continuity Risk
Clinical continuity risk arises where AI becomes part of:
- booking;
- triage;
- routing;
- documentation;
- summarisation;
- referral generation;
- patient messaging;
- and administrative scheduling.
If the system fails, is withdrawn, is inaccessible, or becomes legally restricted, the NHS must still be able to provide care.
The continuity plan must show:
- fallback routes;
- manual processes;
- staff capacity;
- data export;
- record access;
- audit preservation;
- patient communication;
- incident response;
- and safe rollback.
Without that, dependency becomes a patient-safety risk.
Data Portability and Record Integrity Risk
If AI systems generate notes, summaries, logs, triage outputs, prompts, or audit events, exit requires more than exporting patient records.
The NHS must preserve:
- source input;
- AI output;
- transcript;
- final note;
- edit history;
- model version;
- audit log;
- correction history;
- consent record;
- objection record;
- support record;
- and incident record.
Otherwise, exit may break evidential continuity.
A future complaint, tribunal, negligence claim, subject access request, correction request, or regulatory investigation may require records created by the old AI system.
If those records remain trapped inside vendor infrastructure, accountability is weakened.
Public-Law Risk
A public body must act rationally, proportionately, transparently, and in accordance with relevant duties.
Where a public healthcare system becomes dependent on AI infrastructure, the public-law questions are:
- Was the dependency assessed?
- Were alternatives considered?
- Was lock-in considered?
- Was exit cost considered?
- Was sovereign control considered?
- Was patient access risk considered?
- Was equality impact considered?
- Was data execution considered?
- Was public consultation required?
- Was procurement transparent?
- Was the risk of future service withdrawal assessed?
A rollout can be technologically ambitious while still legally weak if dependency risk is not assessed.
Workforce Dependency Risk
Staff may become dependent on AI tools because workload, staffing levels, productivity targets, and management expectations adapt around AI outputs.
The risk chain is:
AI saves time claim → workload expectations change → staff rely on AI → AI withdrawn or degraded → workload becomes unsafe → staff blamed for failure
This creates employment and health-and-safety risk.
The employer must not use AI productivity claims to increase demand before proving the system is reliable, reversible, and properly supported.
Patient Access Dependency Risk
Patients may become dependent on AI access routes where:
- app triage becomes the normal route;
- phone routes are reduced;
- reception capacity is reduced;
- self-care routing increases;
- appointment booking shifts online;
- triage outputs drive access priority;
- and non-digital fallback becomes slower.
That creates the risk:
AI route fails → patient cannot reach equivalent care
Universal healthcare cannot depend on a digital route that is not guaranteed, reversible, accessible, and human-fallback safe.
Tribunal / Procedural Risk
This breach has tribunal and procedural relevance because dependency records may be needed in future disputes.
Where AI systems are used in employment, clinical, data, negligence, equality, protected-disclosure, or public-law proceedings, the affected party may need:
- procurement record;
- contract terms;
- exit plan;
- DPIA;
- clinical safety case;
- equality assessment;
- data export plan;
- processor and sub-processor map;
- model version history;
- audit logs;
- support records;
- continuity plan;
- and incident records.
If dependency prevents access to historical records, the AI system undermines procedural fairness.
Disclosure Questions
- What sovereign exit plan exists for Microsoft 365 Copilot deployment?
- What sovereign exit plan exists for NHS App AI triage?
- What sovereign exit plan exists for ambient voice / AI scribing systems?
- What fallback exists if a vendor withdraws service?
- What fallback exists if pricing changes after dependency forms?
- What fallback exists if access is suspended?
- What fallback exists if model behaviour changes?
- What fallback exists if legal restrictions affect service availability?
- Can the NHS export prompts, outputs, summaries, logs, telemetry, and audit trails?
- Can the NHS preserve model version history after exit?
- Can the NHS reconstruct AI decisions after exit?
- Can patient records remain complete after vendor exit?
- Can disciplinary or tribunal evidence be produced after vendor exit?
- Can subject access requests be answered after vendor exit?
- Can rectification requests be answered after vendor exit?
- Can clinical incidents be investigated after vendor exit?
- What open standards are used?
- What interoperability testing has been completed?
- What data-portability plan exists?
- What manual fallback capacity exists?
- What non-AI patient-access route is protected?
- What non-vendor clinical documentation route remains?
- What staffing model exists if AI is withdrawn?
- What continuity test has been run?
- What disaster-recovery test has been run?
- What vendor lock-in assessment exists?
- What public procurement assessment considered dependency?
- What parliamentary or public scrutiny considered AI dependency?
- What sovereign alternative was assessed?
- What public document proves the NHS can exit safely?
Evidence Relied Upon
EX-B18-01 — NHS England announcement that more than 500,000 staff are to receive Microsoft 365 Copilot following a 30,000-worker trial across 90 NHS organisations and claimed 43-minute daily savings. (NHS England)
EX-B18-02 — Microsoft statement describing NHS England’s Microsoft 365 Copilot adoption as a service-delivery, cost-reduction, and care-time initiative. (Source)
EX-B18-03 — NHS England announcement that NHS App AI triage is being rolled out to over 200,000 patients within 12 months and all NHS App users by April 2028. (NHS England)
EX-B18-04 — NHS England ambient scribing guidance describing generative-AI ambient voice technologies for clinical or patient documentation and workflow support. (NHS England)
EX-B18-05 — NHS Digital IG guidance for AI-enabled ambient scribing products for patients, staff and IG professionals. (NHS England Digital)
Final Breach Position
This breach records that NHS AI deployment creates public-sector dependency risk where patient access, staff productivity, clinical documentation, audit trails, triage routing, and administrative workflows become reliant on AI, SaaS, cloud, vendor, and proprietary model infrastructure.
The legal issue is not whether external technology can be used.
The legal issue is whether the NHS has proven that it can exit, replace, audit, continue, and preserve records without loss of patient access, clinical safety, data rights, staff fairness, or public accountability.
Until that is shown, the rollout remains structurally dependent.
Core line:
AI dependency without a sovereign exit plan is not transformation. It is operational capture.
Consolidated Breach Conclusion — NHS AI Disclosure Position
Summary
The 18 breaches establish one combined public-interest disclosure.
This is not a single technical objection.
It is a national governance failure pattern.
The pattern is:
AI rollout → patient data exposure → staff liability exposure → opaque processing → unclear consent → weak traceability → unequal access risk → vendor dependency → missing public assurance
The combined disclosure position is:
NHS AI systems are being advanced across patient access, clinical documentation, staff workflow, triage, ambient voice, audit, and administration before the public record visibly proves lawful execution, safety, transparency, equality, consent, sovereignty, accountability, and reversibility.
Consolidated Breach Pattern
The breaches operate as one chain:
- Staff are publicly threatened with dismissal or prison while institutional AI systems expand around them.
- Named AI licences create worker-identifiable audit trails that may later be used in discipline or tribunal proceedings.
- AI triage creates a patient-access decision layer without visible disclosure of the processing engine.
- Storage location is substituted for execution disclosure, leaving model, inference, telemetry, support, and data-bleed questions unresolved.
- AI triage outputs may affect care routing without visible source-to-output traceability.
- Accent, dialect, speech, language, disability, and clinical-noise validation is not visibly proven at national scale.
- Ambient voice places AI between the spoken consultation and the official medical record.
- Patient consent and meaningful choice are not visibly settled.
- Pseudonymisation does not resolve AI-era re-identification risk.
- Staff competence and AI training appear mismatched against rollout speed and liability exposure.
- Clinical safety, DPIA, equality, accessibility, and algorithmic assurance are not visibly complete.
- Digital-first AI access risks excluding patients who cannot use or safely trust the route.
- Cybersecurity is incomplete if it ignores authorised-use exposure and AI exhaust.
- AI output creates verification burden, stress, and liability transfer onto workers.
- Vendor, sub-processor, cloud, telemetry, and support-access chains are not visibly mapped.
- Accountability is fragmented between NHS England, ICBs, GP practices, vendors, staff, and cloud providers.
- AI-derived material may become evidence before its chain is disclosed.
- Public-sector AI dependency forms before sovereign exit and continuity are proven.
Central Finding
The central finding is:
The NHS AI rollout is not merely a digital transformation programme. It is a new processing architecture for patient access, medical records, workforce conduct, clinical documentation, administrative decision-making, and evidential record creation.
That means it cannot be governed through ordinary IT language.
It requires full disclosure of:
- execution location;
- model logic;
- clinical safety case;
- DPIA;
- equality assessment;
- accessibility assessment;
- algorithmic transparency record;
- vendor chain;
- sub-processor chain;
- telemetry route;
- support-access route;
- patient consent route;
- staff training route;
- audit-log use;
- tribunal evidence use;
- data-bleed controls;
- re-identification controls;
- and sovereign exit plan.
Core Public-Interest Statement
This disclosure is made because NHS AI systems may affect:
- how patients access care;
- how symptoms are classified;
- how urgency is assigned;
- how appointments are routed;
- how clinical consultations are recorded;
- how patient speech becomes documentation;
- how staff use AI;
- how staff are audited;
- how staff may be disciplined;
- how medical records are formed;
- how patient data is processed;
- how logs and telemetry are generated;
- how vendors and cloud providers gain operational roles;
- how AI-derived records may enter tribunals or complaints;
- and how public-sector dependency becomes structurally embedded.
The issue is therefore not speculative.
The issue is structural.
Unified Legal Position
The combined legal position is:
No public healthcare AI system should be deployed at national scale unless the deploying public bodies can prove that the system is lawful, safe, transparent, auditable, accountable, equal, clinically governed, reversible, and sovereignly controllable.
Where the system affects patient access or clinical records, the threshold is higher.
Where the system processes special-category health data, the threshold is higher.
Where the system creates staff audit trails or disciplinary exposure, the threshold is higher.
Where the system introduces foreign-controlled infrastructure, vendor dependency, cloud processing, telemetry, or model execution, the threshold is higher.
Where the system may generate evidence, the threshold is higher.
Consolidated Disclosure Demands
The following disclosures are required.
1. Full AI System Register
Publish a register identifying every AI, automated, generative, triage, ambient voice, scribing, Copilot-style, SaaS, workflow, clinical-documentation, and patient-access system being deployed.
For each system, disclose:
- name;
- vendor;
- purpose;
- NHS organisation using it;
- patient or staff population affected;
- data processed;
- outputs generated;
- human-review pathway;
- and deployment status.
2. Execution and Processing Map
Publish a full execution map showing:
- where patient data is stored;
- where it is processed;
- where inference occurs;
- where speech-to-text occurs;
- where summarisation occurs;
- where triage logic executes;
- where logs are processed;
- where telemetry is processed;
- where model monitoring occurs;
- where support access occurs;
- where backup and disaster recovery operate;
- and whether any non-UK jurisdiction is involved.
Core requirement:
Storage map is not enough. Execution map is required.
3. Vendor and Sub-Processor Map
Publish a full chain showing:
- controller;
- joint controller if applicable;
- processor;
- sub-processors;
- cloud provider;
- AI model provider;
- speech-to-text provider;
- analytics provider;
- telemetry provider;
- support provider;
- backup provider;
- disaster recovery provider;
- and legal jurisdictions engaged.
4. Clinical Safety Evidence
Publish or identify the clinical safety evidence for each AI system affecting patient access, clinical workflow, triage, documentation, or record formation.
This must include:
- DCB0129 evidence;
- DCB0160 evidence;
- clinical safety case;
- hazard log;
- residual risk approval;
- clinical safety officer;
- incident route;
- under-triage controls;
- false reassurance controls;
- ambient voice error controls;
- and post-deployment monitoring.
5. DPIA and Data Protection Evidence
Publish or identify DPIAs covering:
- AI triage;
- ambient voice;
- AI scribing;
- Copilot-style staff AI tools;
- patient-access AI;
- AI logs;
- telemetry;
- support access;
- model monitoring;
- cross-border data flow;
- re-identification risk;
- and staff audit-trail exposure.
6. Equality and Accessibility Evidence
Publish or identify equality and accessibility assessments covering:
- disability;
- age;
- race;
- language;
- nationality;
- accent;
- digital exclusion;
- poverty;
- neurodivergence;
- sensory impairment;
- health literacy;
- shared-device risk;
- domestic abuse / coercive control;
- safeguarding-sensitive disclosure;
- and equivalent non-AI access.
7. Patient Consent and Objection Route
Publish a clear patient-facing AI notice explaining:
- when AI is used;
- what AI does;
- whether AI affects routing or record formation;
- whether voice is captured;
- whether audio is retained;
- whether transcripts are retained;
- whether AI-generated notes are retained;
- whether data is used for model improvement;
- whether data crosses borders;
- how to refuse;
- how to object;
- how to correct errors;
- and how equivalent care remains available without AI.
8. Staff Training and Liability Protection
Publish staff-facing governance showing:
- training completed before AI exposure;
- role-specific AI-use rules;
- patient-data input rules;
- prohibited-use rules;
- verification duties;
- hallucination/error handling;
- audit-log consequences;
- disciplinary-use boundaries;
- protected-disclosure route;
- stress risk assessment;
- equality-adjusted training;
- and worker protection where AI error originates upstream.
9. AI Evidence Protocol
Publish a protocol governing the use of AI-derived material in:
- HR investigations;
- disciplinary proceedings;
- employment tribunals;
- clinical complaints;
- negligence disputes;
- data-protection complaints;
- professional-regulation referrals;
- coronial proceedings;
- and protected-disclosure matters.
The protocol must require disclosure of:
- prompt;
- source material;
- AI output;
- draft versions;
- final version;
- edit history;
- model version;
- system version;
- timestamp logic;
- user identity;
- audit logs;
- human-review record;
- correction history;
- and vendor / processor chain.
10. Sovereign Exit and Continuity Plan
Publish an exit and continuity plan proving that NHS services can continue if:
- vendor service is withdrawn;
- pricing changes;
- licence terms change;
- access is suspended;
- cloud service degrades;
- model behaviour changes;
- legal restrictions arise;
- support location changes;
- telemetry rules change;
- or a sovereign replacement becomes necessary.
The plan must preserve:
- patient access;
- clinical records;
- audit trails;
- subject access rights;
- correction rights;
- tribunal evidence;
- patient complaints;
- staff disciplinary records;
- and clinical incident investigation.
Consolidated Remedy Sought
The remedy sought is not the rejection of all technology.
The remedy sought is lawful deployment.
That requires:
- Immediate publication of AI system registers.
- Publication of execution and processing maps.
- Publication of vendor and sub-processor chains.
- Publication of clinical safety assurance.
- Publication of DPIAs and equality assessments.
- Clear patient AI consent / objection / equivalent-access route.
- Clear staff training and liability protection.
- Restriction on disciplinary reliance on AI material until AI evidence protocols exist.
- Restriction on patient-record reliance where ambient voice chains are incomplete.
- Restriction on national scaling where accent, language, disability, and digital exclusion validation remains unpublished.
- Publication of sovereign exit and continuity plan.
- Independent public audit of NHS AI deployment before full national reliance forms.
Final Disclosure Position
This disclosure records that NHS AI deployment has crossed from ordinary IT support into public healthcare infrastructure.
Once AI systems affect patient access, clinical documentation, staff workflow, audit trails, evidence creation, and operational capacity, they must be treated as legal infrastructure.
The public must be shown the complete chain.
Not slogans.
Not productivity claims.
Not storage assurances.
Not pilot headlines.
The complete chain.
Patient input → system execution → model output → human review → record consequence → audit trail → vendor chain → legal accountability → exit route
Until that chain is visible, the NHS AI rollout remains legally unresolved.
Final core line:
The NHS cannot lawfully build the future of public healthcare on AI systems whose execution, evidence, accountability, consent, safety, and exit routes remain hidden.
Legal and Human Rights Frameworks Engaged
This section examines the legal and human-rights frameworks engaged by the NHS AI deployment issues recorded in this disclosure.
The disclosure concerns the introduction of AI systems into NHS healthcare environments where patient symptoms, medical records, consultation speech, triage answers, clinical notes, staff prompts, audit logs, telemetry, AI-generated summaries, access histories, and system outputs may be processed, retained, reviewed, relied upon, or exposed through AI, SaaS, cloud, vendor-support, model-monitoring, and externally administered processing chains.
The case is not limited to whether NHS bodies have a general power to process patient data.
The issue is whether NHS AI deployment alters the confidential medical relationship by inserting automated, externally supported, or non-sovereign processing layers between the patient, the clinician, the record, the worker, the audit trail, and any later evidential reliance.
The frameworks addressed below include:
- Magna Carta principles concerning lawful process, arbitrary institutional interference, and unsupported official assertion;
- Canon Law confidentiality principles concerning protected disclosure inside a trust relationship;
- Common Law confidentiality and privacy protections, including medical confidentiality, breach of confidence, and misuse of private information;
- Human Rights Act 1998 and Convention rights, including public-authority compatibility, private life, dignity, and non-discrimination;
- Equality Act 2010 duties, including indirect discrimination, reasonable adjustments, services and public functions, and the Public Sector Equality Duty;
- NHS Constitution rights, including privacy, confidentiality, patient involvement, dignity, safe care, and patient trust;
- Caldicott Principles, including necessity, minimisation, need-to-know access, lawful use, staff responsibility, and patient information;
- UK GDPR and Data Protection Act 2018 provisions, including lawfulness, fairness, transparency, special-category health data, data-subject rights, security, DPIAs, processor controls, re-identification, preservation, and international-transfer safeguards;
- NHS Clinical Safety and Health IT Governance Standards (including DCB0129, DCB0160 and DTAC), medical-device assessment, records management, clinical-risk management, and duty of candour;
- Employment, Whistleblowing, Staff Safety and Workplace Law, including protected disclosure, unfair dismissal, health and safety, stress risk, disciplinary fairness, and AI-derived staff audit exposure;
- Public Law duties, including rationality, proportionality, procedural fairness, legitimate expectation, procurement accountability, value for money, continuity, resilience, and sovereign exit risk;
- Evidential and Procedural Safeguards, including AI-generated material, source-to-output traceability, disclosure, preservation, tribunal fairness, litigation prejudice, and evidential reliability;
- Universal Declaration of Human Rights (UDHR) principles;
- International Covenant on Civil and Political Rights (ICCPR) principles;
- International Covenant on Economic, Social and Cultural Rights (ICESCR) principles;
- Council of Europe Convention 108+ principles;
- OECD AI Principles on trustworthy AI and responsible data governance;
- UNESCO Recommendation on the Ethics of Artificial Intelligence principles;
- United Nations Guiding Principles on Business and Human Rights (UNGPs);
- International Privacy and Data Protection Principles;
- International Bioethical Principles concerning dignity, consent, confidentiality, equality, autonomy, medical identity, and responsible institutional processing.
The disclosure identifies NHS AI deployment as a layered legal issue concerning medical confidentiality, patient autonomy, clinical safety, staff exposure, public accountability, evidential reliability, equality of access, and sovereign control over critical healthcare infrastructure.
The central concern is that confidential medical information and worker data may be converted into AI outputs, summaries, classifications, logs, telemetry, audit trails, and evidence-capable records before the public has been shown the full processing pathway, vendor chain, safety case, equality assessment, objection route, correction route, accountability map, and exit plan.
Legal Frameworks Engaged.
I.1 Magna Carta 1215 — Law of the Land / Protection Against Arbitrary Interference
Source:
Magna Carta 1215, Clause 39.
Material source: National Archives — Magna Carta 1215, British Library Magna Carta, Runnymede.
URL: https://www.nationalarchives.gov.uk/education/resources/magna-carta/british-library-magna-carta-1215-runnymede/
Verbatim / principle:
“No free man shall be seized or imprisoned, or stripped of his rights or possessions, or outlawed or exiled, or deprived of his standing in any way… except by the lawful judgment of his equals or by the law of the land.”
Analysis:
The disclosure identifies Magna Carta as part of the historical constitutional lineage protecting the person from arbitrary institutional interference.
The disclosure does not rely on Magna Carta as a modern standalone data-protection statute.
It relies on the continuing constitutional principle that institutional power over the person must be justified by lawful authority, lawful process, proportionality, and accountable governance.
NHS AI deployment engages this lineage where patient medical identity, confidential health information, clinical access routes, AI-generated records, and staff audit trails are placed inside systems whose processing pathway, access chain, evidential status, and sovereign-control structure are not fully visible.
The concern is not merely data processing.
The concern is arbitrary institutional interference with the person through medical identity, private information, access to care, and AI-derived records unless justified by law, safeguards, and transparent process.
I.2 Magna Carta 1215 — Unsupported Official Assertion and Evidential Foundation
Source:
Magna Carta 1215, Clause 38.
Material source: National Archives — Magna Carta 1215, British Library Magna Carta, Runnymede.
URL: https://www.nationalarchives.gov.uk/education/resources/magna-carta/british-library-magna-carta-1215-runnymede/
Verbatim / principle:
“In future no official shall place a man on trial upon his own unsupported statement, without producing credible witnesses to the truth of it.”
Analysis:
The disclosure identifies Clause 38 as part of the historical evidential lineage requiring official assertion to be supported by credible proof.
This principle is engaged by NHS AI deployment where AI-generated material may later be treated as record, audit trail, disciplinary evidence, clinical evidence, tribunal evidence, complaint evidence, or regulatory evidence.
The disclosure asserts that AI-derived material cannot be treated as self-proving.
Where AI systems generate summaries, transcripts, triage outputs, staff-use logs, access records, model-monitoring signals, audit trails, or evidential records, the affected person must be able to test the source, prompt, model version, human review, edit history, timestamp, system configuration, and processing chain.
The constitutional concern is that institutional AI output must not become official truth without a traceable evidential foundation.
I.3 Canon Law — Confessional Confidentiality and Protected Disclosure
Source:
Code of Canon Law, Canon 983 §1 — sacramental seal / seal of confession.
Material source: Vatican — Code of Canon Law, Book IV, Cann. 959–997.
URL: https://www.vatican.va/archive/cod-iuris-canonici/eng/documents/cic_lib4-cann959-997_en.html
Verbatim / principle:
“The sacramental seal is inviolable; therefore it is absolutely forbidden for a confessor to betray in any way a penitent in words or in any manner and for any reason.”
Analysis:
The disclosure identifies canon-law confidentiality as part of the historical privacy and confidentiality lineage preceding modern professional confidentiality doctrines.
The principle is not relied upon as NHS statutory law.
It is relied upon as historical evidence that certain disclosures are made inside protected trust relationships and must not be exposed to external power.
Medical disclosure belongs within that same protected logic.
Patients disclose intimate matters concerning the body, mind, disease, disability, sexuality, abuse, addiction, mortality, family, genetics, mental health, fear, shame, and vulnerability.
The disclosure therefore identifies NHS AI deployment as engaging the ancient confidentiality principle where intimate medical disclosures are captured, transcribed, summarised, logged, analysed, routed, or retained through AI, SaaS, cloud, telemetry, vendor-support, model-monitoring, or external processing environments.
The principle is that confidential disclosure creates a protected trust boundary.
II. Common Law — Confidentiality and Privacy Layer
II.1 Common Law Duty of Confidentiality
Source:
Common law medical confidentiality doctrine; Hunter v Mann [1974] QB 767.
Material source: Hunter v Mann principle as cited in UK medical confidentiality law and professional guidance.
URL: https://www.bailii.org/
Verbatim / principle:
“The doctor is under a duty not to disclose, without the consent of the patient, information which he, the doctor, has gained in his professional capacity…”
Analysis:
The disclosure identifies that patients disclose intimate medical information within a confidential healthcare relationship.
That relationship is not created for open-ended AI processing, externalised SaaS execution, vendor support access, telemetry generation, model monitoring, staff audit exposure, or secondary evidential use.
The disclosure asserts that NHS AI deployment engages the common law duty of confidentiality where symptom data, voice data, triage answers, clinical notes, medication information, disability information, mental-health disclosures, safeguarding material, and AI-generated summaries are processed through systems whose complete access, execution, logging, retention, vendor, support, and correction pathways have not been made visibly clear.
The confidentiality concern is therefore not limited to publication or obvious disclosure.
It extends to the movement of confidential medical information into AI-mediated processing environments that may materially exceed the patient’s reasonable expectation of confidential healthcare use.
II.2 Breach of Confidence
Source:
Common law / equitable doctrine of confidence.
Material source: Coco v A N Clark (Engineers) Ltd [1969] RPC 41; Attorney General v Guardian Newspapers Ltd (No 2) [1990] 1 AC 109.
URL: https://www.bailii.org/
Verbatim / principle:
Information imparted in circumstances importing an obligation of confidence must not be used or disclosed without authority in a manner inconsistent with that confidence.
Analysis:
The disclosure identifies that medical information supplied to NHS clinicians, GP systems, NHS App pathways, triage routes, and healthcare services is imparted in circumstances importing an obligation of confidence.
The disclosure asserts that AI deployment may create breach-of-confidence concerns where confidential medical information is reused, transformed, logged, summarised, transcribed, exposed, monitored, or made available through external AI, SaaS, cloud, telemetry, support, or model-monitoring systems beyond the confidential care purpose.
The issue is not whether the NHS may process patient data for care.
The issue is whether AI processing alters the use environment so materially that confidential information is handled in a way not reasonably understood or authorised by the patient.
The disclosure therefore identifies breach-of-confidence risk where confidential medical data is processed through widened AI infrastructure without clear authority, necessity, proportionality, transparency, and safeguard.
II.3 Misuse of Private Information
Source:
Common law privacy tort; misuse of private information.
Material source: Campbell v MGN Ltd [2004] UKHL 22; Google Inc v Vidal-Hall [2015] EWCA Civ 311.
URL: https://www.bailii.org/
Verbatim / principle:
A person may have a reasonable expectation of privacy in information concerning private life, health, correspondence, identity, dignity, and personal autonomy.
Analysis:
The disclosure identifies NHS medical data as carrying a heightened reasonable expectation of privacy.
That expectation applies to symptoms, diagnosis, medication, disability information, mental-health disclosures, safeguarding material, clinical history, consultation speech, triage answers, appointment behaviour, AI-generated summaries, transcripts, and inferred clinical meaning.
The disclosure asserts that AI systems may create misuse-of-private-information risk where private medical material is transformed into prompts, outputs, logs, telemetry, summaries, classifications, audit trails, support records, or AI-derived evidence without clear disclosure and meaningful control.
The privacy concern attaches not only to the original medical record.
It attaches to AI-derived material that reveals or reconstructs the same private medical identity.
III.4 Human Rights Act 1998, Schedule 1, Article 6 — Right to a Fair Hearing
Source:
Human Rights Act 1998, Schedule 1, Article 6 — Right to a fair trial.
Material source: legislation.gov.uk — Human Rights Act 1998, Schedule 1, Article 6.
URL: https://www.legislation.gov.uk/ukpga/1998/42/schedule/1/part/I/chapter/5
Verbatim / principle:
“In the determination of his civil rights and obligations… everyone is entitled to a fair and public hearing within a reasonable time by an independent and impartial tribunal established by law.”
Analysis:
The disclosure identifies Article 6 as engaged where AI-generated or AI-mediated material may later be relied upon in employment, disciplinary, clinical, regulatory, tribunal, complaint, negligence, professional-referral, protected-disclosure, or data-rights proceedings.
The relevant material may include AI-generated summaries, ambient voice transcripts, triage outputs, staff prompts, Copilot usage logs, audit trails, telemetry, model-monitoring records, support tickets, generated HR documents, AI-assisted investigation notes, and clinical-record entries.
The disclosure asserts that AI-derived material cannot be fairly relied upon where the affected person cannot inspect, understand, challenge, correct, or test the evidence chain.
The Article 6 concern is that procedural fairness is undermined where AI-generated or AI-mediated records are treated as ordinary evidence while the underlying source, prompt, model, system version, processing pathway, human review, edit history, vendor chain, and audit logic remain undisclosed.
The disclosure therefore identifies that AI-derived material must be traceable, preserved, disclosed, and capable of challenge before it is relied upon in any process affecting civil rights, employment rights, patient rights, professional status, or legal position.
III.5 Human Rights Act 1998, Schedule 1, Article 10 — Freedom of Expression
Source:
Human Rights Act 1998, Schedule 1, Article 10 — Freedom of expression.
Material source: legislation.gov.uk — Human Rights Act 1998, Schedule 1, Article 10.
URL: https://www.legislation.gov.uk/ukpga/1998/42/schedule/1/part/I/chapter/9
Verbatim / principle:
“Everyone has the right to freedom of expression.”“This right shall include freedom to hold opinions and to receive and impart information and ideas without interference by public authority.”
Analysis:
The disclosure identifies Article 10 as engaged where patients, workers, clinicians, whistleblowers, journalists, researchers, litigants, or members of the public raise concerns about NHS AI deployment, patient-data processing, clinical safety, medical confidentiality, equality impact, staff exposure, vendor dependency, or public-sector AI governance.
The disclosure asserts that public-interest speech concerning NHS AI must not be chilled by opaque audit systems, disciplinary pressure, reputational framing, AI-derived staff records, procedural retaliation, or institutional characterisation of legitimate concern as misconduct, disruption, or non-compliance.
The Article 10 concern is intensified where AI systems create records that may later be used to monitor, assess, discipline, or discredit workers or patients who raise concerns.
The disclosure therefore identifies that NHS AI governance must preserve public-interest expression, protected disclosure, patient complaint rights, staff safety reporting, and the ability to receive and impart information concerning risks in public healthcare infrastructure.
III.6 Human Rights Act 1998, Schedule 1, Article 13 — Effective Remedy
Source:
Human Rights Act 1998, Schedule 1, Article 13 — Right to an effective remedy.
Material source: legislation.gov.uk — Human Rights Act 1998, Schedule 1, Article 13.
URL: https://www.legislation.gov.uk/ukpga/1998/42/schedule/1/part/II/chapter/3
Verbatim / principle:
“Everyone whose rights and freedoms as set forth in this Convention are violated shall have an effective remedy before a national authority…”
Analysis:
The disclosure identifies effective-remedy concerns where NHS AI systems affect privacy, confidentiality, equality, access to care, clinical records, staff audit exposure, employment position, or evidential reliability, but the affected person cannot identify the system, obtain the record, challenge the output, correct the error, object to processing, or obtain meaningful review.
The concern applies where AI triage produces routing decisions, ambient voice creates inaccurate summaries, AI-generated notes enter the clinical record, staff prompts or logs become disciplinary material, or vendor-supported systems hold records outside the visible NHS record pathway.
The disclosure asserts that remedy is not effective where the person can only challenge the final visible record while the AI source material, prompt, transcript, output, log, telemetry, support record, model-monitoring record, or audit trail remains hidden.
The Article 13 concern is therefore that NHS AI deployment must include practical remedy routes, including access, explanation, correction, restriction, objection, human review, complaint escalation, disclosure preservation, and accountability mapping across the full AI processing chain.
IV. Equality Act 2010 — Equality and Non-Discrimination Layer
IV.1 Equality Act 2010, Section 6 — Disability
Source:
Equality Act 2010, Section 6 — Disability.
Material source: legislation.gov.uk — Equality Act 2010, Section 6.
URL: https://www.legislation.gov.uk/ukpga/2010/15/section/6
Verbatim / principle:
“A person has a disability if—
(a) P has a physical or mental impairment, and
(b) the impairment has a substantial and long-term adverse effect on P’s ability to carry out normal day-to-day activities.”
Analysis:
The disclosure identifies disability as a central equality framework engaged by NHS AI deployment.
The concern applies where AI triage, NHS App routing, digital-first access, ambient voice capture, automated booking, AI-generated clinical summaries, staff AI tools, and audit systems affect patients or workers with physical impairments, mental-health conditions, neurodivergence, cognitive impairment, sensory impairment, speech impairment, fatigue, medication effects, or fluctuating health conditions.
The disclosure asserts that AI systems may create disability-related disadvantage where they require digital competence, rapid form completion, voice clarity, stable cognition, confidence using apps, ability to review AI-generated records, or ability to challenge system outputs.
The disclosure therefore identifies disability as a threshold legal category requiring specific assessment before NHS AI systems are treated as safe, accessible, fair, or nationally scalable.
IV.2 Equality Act 2010, Section 13 — Direct Discrimination
Source:
Equality Act 2010, Section 13 — Direct discrimination.
Material source: legislation.gov.uk — Equality Act 2010, Section 13.
URL: https://www.legislation.gov.uk/ukpga/2010/15/section/13
Verbatim / principle:
“A person (A) discriminates against another (B) if, because of a protected characteristic, A treats B less favourably than A treats or would treat others.”
Analysis:
The disclosure identifies direct-discrimination risk where patients or workers are treated less favourably because of protected characteristics in the design, deployment, use, interpretation, or enforcement of NHS AI systems.
The concern applies where AI systems or human operators using AI outputs treat people differently because of disability, race, age, sex, pregnancy or maternity, religion or belief, sexual orientation, gender reassignment, marriage or civil partnership, nationality-linked language, accent, or ethnicity-linked communication patterns.
The disclosure further identifies that direct discrimination may arise where AI-derived material reinforces assumptions about competence, reliability, risk, communication, access behaviour, non-compliance, aggression, confusion, or credibility.
The disclosure therefore identifies that NHS AI outputs, summaries, triage classifications, staff audit logs, and disciplinary records must not become automated routes for less favourable treatment connected to protected characteristics.
IV.3 Equality Act 2010, Section 15 — Discrimination Arising From Disability
Source:
Equality Act 2010, Section 15 — Discrimination arising from disability.
Material source: legislation.gov.uk — Equality Act 2010, Section 15.
URL: https://www.legislation.gov.uk/ukpga/2010/15/section/15
Verbatim / principle:
“A person (A) discriminates against a disabled person (B) if—
(a) A treats B unfavourably because of something arising in consequence of B’s disability, and
(b) A cannot show that the treatment is a proportionate means of achieving a legitimate aim.”
Analysis:
The disclosure identifies that NHS AI deployment may create unfavourable treatment arising from disability where disabled patients or workers struggle with AI-mediated systems because of impairment-related effects.
The concern applies where a patient cannot complete digital triage because of cognitive impairment, cannot use app-based access because of visual impairment, cannot communicate safely through voice capture because of speech impairment, cannot review AI-generated summaries because of fatigue or neurodivergence, or cannot challenge inaccurate AI records because of health limitation.
The concern also applies where staff are judged negatively because disability affects AI tool use, prompt-writing speed, verification pace, training completion, audit patterns, or interaction with AI-generated workflows.
The disclosure asserts that NHS AI systems must not treat disability-related difficulty as non-compliance, poor engagement, reduced competence, failure to cooperate, or misconduct.
The disclosure therefore identifies Section 15 as engaged wherever AI-mediated disadvantage arises from disability-related need, limitation, communication difference, or adjustment requirement.
IV.4 Equality Act 2010, Section 19 — Indirect Discrimination
Source:
Equality Act 2010, Section 19 — Indirect discrimination.
Material source: legislation.gov.uk — Equality Act 2010, Section 19.
URL: https://www.legislation.gov.uk/ukpga/2010/15/section/19
Verbatim / principle:
“A person (A) discriminates against another (B) if A applies to B a provision, criterion or practice which is discriminatory in relation to a relevant protected characteristic.”
Analysis:
The disclosure identifies NHS AI triage, NHS App routing, digital-first access, ambient voice technology, AI scribing, speech recognition, staff AI tools, audit logs, and AI training requirements as provisions, criteria, or practices capable of producing unequal effects.
The disclosure asserts that these systems may appear neutral while disadvantaging people by disability, age, race, language, nationality, accent, ethnicity, sensory impairment, neurodivergence, digital exclusion, poverty, health literacy, or communication need.
The concern applies where patients cannot complete AI triage, cannot safely use app-based access, are mistranscribed by speech systems, are routed incorrectly because of communication difference, or are given poorer access because human alternatives are reduced.
The disclosure therefore identifies indirect-discrimination risk where AI-mediated healthcare access creates unequal burden, unequal error exposure, unequal verification demand, or unequal access to redress.
IV.5 Equality Act 2010, Sections 20–21 — Duty to Make Reasonable Adjustments
Source:
Equality Act 2010, Sections 20–21 — Duty to make reasonable adjustments.
Material source: legislation.gov.uk — Equality Act 2010, Sections 20 and 21.
URL: https://www.legislation.gov.uk/ukpga/2010/15/section/20
URL: https://www.legislation.gov.uk/ukpga/2010/15/section/21
Verbatim / principle:
“Where this Act imposes a duty to make reasonable adjustments on a person, this section… applies.”“A failure to comply with the first, second or third requirement is a failure to comply with a duty to make reasonable adjustments.”
Analysis:
The disclosure identifies that AI-mediated healthcare routes must not place disabled patients or workers at substantial disadvantage by making AI, digital triage, voice capture, app-based access, automated routing, AI-generated summaries, or AI-audited workflows the practical gateway to care or work performance without accessible alternatives.
The concern applies to visual impairment, hearing impairment, learning disability, cognitive impairment, neurodivergence, mobility or dexterity impairment, mental-health distress, fatigue, speech impairment, and disability-related communication needs.
The disclosure asserts that reasonable adjustments must include accessible information, non-digital access routes, human assistance, interpreter support, non-voice alternatives, equivalent non-AI routes, staff training adjustments, additional review time, safe objection routes, and protection from audit or disciplinary disadvantage caused by inaccessible AI systems.
The statutory concern is that AI deployment cannot make healthcare access, clinical participation, employment compliance, or record correction conditional on an unadjusted digital or voice-processing route.
IV.6 Equality Act 2010, Section 26 — Harassment
Source:
Equality Act 2010, Section 26 — Harassment.
Material source: legislation.gov.uk — Equality Act 2010, Section 26.
URL: https://www.legislation.gov.uk/ukpga/2010/15/section/26
Verbatim / principle:
“A person (A) harasses another (B) if—
(a) A engages in unwanted conduct related to a relevant protected characteristic, and
(b) the conduct has the purpose or effect of violating B’s dignity, or creating an intimidating, hostile, degrading, humiliating or offensive environment for B.”
Analysis:
The disclosure identifies harassment risk where AI-generated material, audit logs, staff-monitoring outputs, access histories, prompt records, patient-record allegations, or AI-assisted disciplinary documents are used in a way that creates a hostile or degrading environment linked to protected characteristics.
The concern applies to workers and patients where AI-derived outputs mischaracterise communication, disability-related behaviour, accent, language, distress, cognitive difficulty, or protected disclosure as misconduct, aggression, non-compliance, unreliability, or risk.
The disclosure further identifies that public warning language concerning dismissal or criminal consequences for patient-record access may intensify workplace fear where staff are simultaneously required to use AI systems whose audit, access, logging, and responsibility boundaries are unclear.
The disclosure therefore identifies that NHS AI deployment must prevent AI-derived records from becoming tools of dignity harm, protected-characteristic hostility, or intimidating institutional pressure.
IV.7 Equality Act 2010, Section 27 — Victimisation
Source:
Equality Act 2010, Section 27 — Victimisation.
Material source: legislation.gov.uk — Equality Act 2010, Section 27.
URL: https://www.legislation.gov.uk/ukpga/2010/15/section/27
Verbatim / principle:
“A person (A) victimises another person (B) if A subjects B to a detriment because—
(a) B does a protected act, or
(b) A believes that B has done, or may do, a protected act.”
Analysis:
The disclosure identifies victimisation risk where patients or workers raise equality concerns about NHS AI systems and are later subjected to detriment through AI-derived records, audit histories, access logs, staff-use data, disciplinary material, complaint handling, or adverse institutional characterisation.
The concern applies where a worker complains that an AI system disadvantages disabled patients, mistranscribes accented speech, excludes digitally disadvantaged groups, or creates discriminatory audit exposure, and is then monitored, disciplined, isolated, or criticised using AI-generated or AI-logged material.
The concern also applies where a patient complains about inaccessible AI triage, lack of reasonable adjustments, discriminatory routing, or inaccurate AI-generated clinical records and is later treated as difficult, non-compliant, disruptive, or procedurally burdensome.
The disclosure therefore identifies that equality complaints about NHS AI must be protected from retaliatory use of AI-derived records.
IV.8 Equality Act 2010, Section 29 — Services and Public Functions
Source:
Equality Act 2010, Section 29 — Provision of services and public functions.
Material source: legislation.gov.uk — Equality Act 2010, Section 29.
URL: https://www.legislation.gov.uk/ukpga/2010/15/section/29
Verbatim / principle:
“A person concerned with the provision of a service to the public or a section of the public… must not discriminate against a person requiring the service.”
Analysis:
The disclosure identifies NHS AI triage, NHS App routing, GP access tools, ambient voice systems, AI scribing products, automated appointment pathways, and digital-first healthcare routes as systems operating inside the provision of public healthcare services.
The concern is that once AI becomes part of the practical route to care, discrimination inside the AI pathway becomes discrimination inside the service.
The disclosure identifies service-risk where patients are delayed, misrouted, under-triaged, excluded, mistranscribed, unable to object, unable to access non-digital alternatives, unable to correct AI-derived records, or given poorer routes because they cannot safely use AI.
The disclosure therefore identifies that NHS AI systems must preserve equal public-service access, not merely offer digital convenience to those able to use it.
IV.9 Equality Act 2010, Section 149 — Public Sector Equality Duty
Source:
Equality Act 2010, Section 149 — Public Sector Equality Duty.
Material source: legislation.gov.uk — Equality Act 2010, Section 149.
URL: https://www.legislation.gov.uk/ukpga/2010/15/section/149
Verbatim / principle:
A public authority must, in the exercise of its functions, have due regard to the need to eliminate discrimination, advance equality of opportunity, and foster good relations.
Analysis:
The disclosure identifies NHS AI deployment as a public function affecting patient access, clinical documentation, confidential medical data, staff workflow, audit exposure, and public trust.
The Public Sector Equality Duty is engaged because AI systems may affect groups differently across disability, age, race, language, accent, national origin, sensory impairment, neurodivergence, health literacy, digital exclusion, and poverty.
The disclosure asserts that equality assessment must precede deployment, not follow harm.
The required assessment must consider app completion rates, abandonment rates, under-triage rates, misrouting rates, speech-recognition error rates, ambient voice transcription errors, accessibility barriers, reasonable-adjustment routes, staff AI-literacy disparities, protected-disclosure risk, and disciplinary exposure caused by unequal competence or system accuracy.
The disclosure therefore identifies that NHS England and deploying bodies must show equality impact analysis rather than rely on general claims that AI improves access.
V. NHS Constitution — Patient Rights, Confidentiality, and Safe Care Layer
V.1 NHS Constitution — Privacy and Confidentiality
Source:
NHS Constitution for England — privacy and confidentiality rights.
Material source: GOV.UK — The NHS Constitution for England.
URL: https://www.gov.uk/government/publications/the-nhs-constitution-for-england/the-nhs-constitution-for-england
Verbatim / principle:
“You have the right to privacy and confidentiality and to expect the NHS to keep your confidential information safe and secure.”
Analysis:
The disclosure identifies a direct conflict between patient expectations under the NHS Constitution and the deployment of AI-mediated processing environments involving triage systems, ambient voice tools, AI-generated clinical summaries, staff-facing AI workflows, cloud infrastructure, telemetry, audit logs, vendor support, and externally administered processing chains.
The disclosure asserts that patients disclose medical information to obtain care, not to have intimate medical identity structures transformed into opaque AI outputs, operational logs, model-monitoring data, support tickets, or evidence-capable records without clear understanding.
The NHS Constitution concern is that safe and secure handling of confidential information must include the full AI processing chain, not only the final medical record or storage location.
The disclosure therefore identifies that NHS AI deployment must preserve patient trust by disclosing how confidential information is captured, processed, transformed, retained, accessed, corrected, audited, and protected.
V.2 NHS Constitution — Involvement in Healthcare Decisions
Source:
NHS Constitution for England — patient involvement in care and treatment.
Material source: GOV.UK — The NHS Constitution for England.
URL: https://www.gov.uk/government/publications/the-nhs-constitution-for-england/the-nhs-constitution-for-england
Verbatim / principle:
“You have the right to be involved in discussions and decisions about your health and care.”
Analysis:
The disclosure identifies that AI triage, automated routing, adaptive questioning, ambient voice capture, AI-generated clinical summaries, and digital-first patient-access systems may affect decisions about patient care before the patient understands the AI role.
The disclosure further identifies that meaningful involvement is undermined where patients are not clearly told whether AI is processing their symptoms, whether AI affects routing, whether AI-generated summaries enter the medical record, whether voice is captured, whether transcripts are retained, or whether equivalent non-AI routes exist.
The NHS Constitution concern is that involvement in healthcare decisions cannot be reduced to passive app use or non-objection to a general notice.
The disclosure therefore identifies that patients must be given clear, accessible, timely information and a meaningful opportunity to object, refuse, correct, or seek human review where AI systems affect access or records.
V.3 NHS Constitution — Safe and Appropriate Care
Source:
NHS Constitution for England — rights relating to care, treatment, safety, and dignity.
Material source: GOV.UK — The NHS Constitution for England.
URL: https://www.gov.uk/government/publications/the-nhs-constitution-for-england/the-nhs-constitution-for-england
Verbatim / principle:
“You have the right to receive care and treatment that is appropriate to you, meets your needs and reflects your preferences.”
Analysis:
The disclosure identifies that AI triage and AI-mediated care access may affect whether a patient is routed to GP, pharmacy, A&E, self-care, community service, urgent review, delayed appointment, or digital-only advice.
The disclosure further identifies that ambient voice and AI scribing may affect the content of the clinical record, which may then influence future treatment.
The safe-care concern is that AI systems must not produce routing outputs, summaries, transcripts, or clinical notes that are inaccurate, untraceable, unreviewed, inaccessible, uncorrectable, or biased against particular patient groups.
The disclosure therefore identifies that safe care requires visible clinical safety cases, human-review pathways, source-to-output traceability, escalation thresholds, under-triage controls, record-correction routes, and post-deployment monitoring.
V.4 NHS Constitution — Dignity, Respect, and Compassionate Care
Source:
NHS Constitution for England — dignity, respect, and compassionate care.
Material source: GOV.UK — The NHS Constitution for England.
URL: https://www.gov.uk/government/publications/the-nhs-constitution-for-england/the-nhs-constitution-for-england
Verbatim / principle:
“You have the right to be treated with dignity and respect, in accordance with your human rights.”
Analysis:
The disclosure identifies that dignity and respect are engaged where AI systems mediate patient access, voice capture, symptom disclosure, triage, clinical documentation, and communication with the NHS.
The concern is that patients may be required to disclose intimate symptoms, mental-health concerns, safeguarding risks, disability information, medication issues, or personal medical histories through systems that do not visibly explain the AI role, data use, record consequence, objection route, or human fallback.
The disclosure further identifies that dignity may be degraded where AI systems misclassify distress, mistranscribe speech, misunderstand accent or disability-related communication, reduce human access, or create records that patients cannot easily correct.
The NHS Constitution concern is that AI-mediated healthcare must not convert vulnerable patient disclosure into opaque system processing that weakens dignity, autonomy, or respectful care.
V.5 NHS Constitution — Patient Choice and Access to Services
Source:
NHS Constitution for England — access to NHS services and patient choice.
Material source: GOV.UK — The NHS Constitution for England.
URL: https://www.gov.uk/government/publications/the-nhs-constitution-for-england/the-nhs-constitution-for-england
Verbatim / principle:
Patients have rights concerning access to NHS services and involvement in choices about care.
Analysis:
The disclosure identifies that NHS AI deployment may affect practical access to healthcare services where digital triage, NHS App routing, automated booking, chatbot-style pathways, AI symptom tools, and AI-mediated administrative systems become gateways to care.
The concern is that patient choice becomes illusory if the non-AI route is slower, harder to access, poorly advertised, or treated as exceptional.
The disclosure asserts that AI deployment must not make access depend on digital literacy, device ownership, stable internet access, confidence using apps, ability to type symptoms, willingness to use voice capture, or ability to understand AI-generated routes.
The NHS Constitution concern is that access and choice must remain real, equivalent, accessible, and safe for patients who cannot or do not wish to use AI-mediated routes.
V.6 NHS Constitution — Complaints, Redress, and Patient Voice
Source:
NHS Constitution for England — complaints and redress rights.
Material source: GOV.UK — The NHS Constitution for England.
URL: https://www.gov.uk/government/publications/the-nhs-constitution-for-england/the-nhs-constitution-for-england
Verbatim / principle:
Patients have the right to complain about NHS services and to have complaints dealt with efficiently and properly investigated.
Analysis:
The disclosure identifies that NHS AI deployment creates new complaint and redress issues where the source of harm may sit inside AI triage, ambient voice capture, transcription, summarisation, routing, logging, model monitoring, support access, or vendor-controlled processing.
The concern is that a patient cannot properly complain about an AI-mediated error if the NHS cannot identify the system, retrieve the source material, explain the output, disclose the human-review step, preserve the log, or correct the AI-derived record.
The disclosure therefore identifies that NHS AI complaint handling must include access to AI-specific records, including prompts, outputs, transcripts, triage answers, routing records, audit trails, correction history, system version, and human-review notes where relevant.
V.7 NHS Constitution — Staff Responsibilities and Patient Confidentiality
Source:
NHS Constitution for England — staff responsibilities and NHS values.
Material source: GOV.UK — The NHS Constitution for England.
URL: https://www.gov.uk/government/publications/the-nhs-constitution-for-england/the-nhs-constitution-for-england
Verbatim / principle:
The NHS Constitution records duties and responsibilities owed by staff, patients, and the public within the NHS system.
Analysis:
The disclosure identifies that NHS AI deployment affects staff responsibilities because staff may be required to use AI tools, verify AI outputs, correct AI-generated records, manage patient confidentiality, respond to audit logs, and carry professional responsibility for material generated upstream by AI systems.
The concern is that staff cannot discharge confidentiality, accuracy, safety, and professional duties where AI processing rules, prompt policies, output-reliance rules, telemetry, support access, audit consequences, and disciplinary boundaries are unclear.
The disclosure further identifies that staff must not be made the accountability endpoint for systems designed, procured, configured, monitored, or controlled by upstream institutional and vendor actors.
The NHS Constitution concern is therefore that staff responsibility must be matched by training, system transparency, role clarity, safe workload, and protection from unfair attribution of AI-generated or system-originated error.
VI. Caldicott Principles — Medical Confidentiality Governance Layer
VI.1 Caldicott Principle 1 — Justify the Purpose
Source:
Caldicott Principles — Principle 1, justify the purpose for using confidential information.
Material source: GOV.UK — The Caldicott Principles.
URL: https://www.gov.uk/government/publications/the-caldicott-principles
Verbatim / principle:
“Every proposed use or transfer of confidential information should be clearly defined, scrutinised and documented.”
Analysis:
The disclosure identifies that NHS AI deployment requires clear definition, scrutiny, and documentation of each processing purpose.
The relevant purposes include AI triage, patient routing, ambient voice capture, transcription, summarisation, clinical documentation, staff workflow assistance, audit logging, telemetry, model monitoring, vendor support, system improvement, security monitoring, and evidential retention.
The disclosure asserts that broad labels such as digital transformation, AI support, productivity, improved access, administrative efficiency, or clinical innovation do not satisfy the Caldicott requirement where confidential information enters multiple processing layers.
The disclosure therefore identifies that each AI pathway must be separately justified, documented, and made visible in relation to the confidential information being processed.
VI.2 Caldicott Principle 2 — Do Not Use Confidential Information Unless Necessary
Source:
Caldicott Principles — Principle 2, do not use confidential information unless necessary.
Material source: GOV.UK — The Caldicott Principles.
URL: https://www.gov.uk/government/publications/the-caldicott-principles
Verbatim / principle:
“Don’t use confidential information unless it is necessary.”
Analysis:
The disclosure identifies that NHS AI systems may process confidential patient information in contexts where necessity has not been visibly demonstrated.
The concern applies to patient symptom data entering AI triage, consultation speech entering ambient voice systems, patient-adjacent material entering Copilot-style workflow tools, prompts and outputs being retained, telemetry being generated, support tickets containing operational data, and model-monitoring records capturing clinical meaning.
The disclosure contests whether every AI-processing layer is necessary for the direct care purpose, particularly where logs, telemetry, analytics, support records, model-monitoring records, or improvement signals may persist beyond the immediate patient-care interaction.
The disclosure therefore identifies necessity as a live question across the entire AI chain, not only at the initial care encounter.
VI.3 Caldicott Principle 3 — Use the Minimum Necessary Confidential Information
Source:
Caldicott Principles — Principle 3, use the minimum necessary confidential information.
Material source: GOV.UK — The Caldicott Principles.
URL: https://www.gov.uk/government/publications/the-caldicott-principles
Verbatim / principle:
“Use the minimum necessary confidential information.”
Analysis:
The disclosure identifies that AI systems may expand rather than minimise the amount of confidential information processed.
Ambient voice may capture more than a clinician would otherwise record. AI triage may collect structured symptom sequences. Copilot-style systems may process patient-adjacent documents, emails, notes, prompts, and workflow material. Logs and telemetry may generate secondary data. Support records may reproduce clinical content. Model-monitoring systems may retain outputs, errors, overrides, red flags, or correction events.
The disclosure asserts that minimum necessary use must apply to every layer: input, prompt, transcript, summary, output, log, telemetry, support record, model-monitoring record, audit trail, correction history, and retained system record.
The disclosure therefore identifies minimisation failure where AI systems create data exhaust beyond what is necessary for direct care.
VI.4 Caldicott Principle 4 — Access on a Strict Need-to-Know Basis
Source:
Caldicott Principles — Principle 4, access to confidential information on a strict need-to-know basis.
Material source: GOV.UK — The Caldicott Principles.
URL: https://www.gov.uk/government/publications/the-caldicott-principles
Verbatim / principle:
“Access to confidential information should be on a strict need-to-know basis.”
Analysis:
The disclosure identifies that AI and SaaS architectures may widen access beyond traditional clinical need-to-know boundaries.
The concern applies to vendors, sub-processors, cloud administrators, telemetry providers, support teams, AI model providers, analytics systems, security monitoring services, and organisational staff who may access logs, transcripts, prompts, outputs, support records, audit trails, or model-monitoring material.
The disclosure further identifies that patient trust is destabilised where the patient cannot see who may access AI-generated or AI-derived records.
The disclosure therefore identifies that need-to-know access must be mapped across the complete processing chain, including system exhaust and support access, not only the main clinical database.
VI.5 Caldicott Principle 5 — Everyone Must Understand Their Responsibilities
Source:
Caldicott Principles — Principle 5, everyone with access to confidential information should understand their responsibilities.
Material source: GOV.UK — The Caldicott Principles.
URL: https://www.gov.uk/government/publications/the-caldicott-principles
Verbatim / principle:
“Everyone with access to confidential information should understand their responsibilities.”
Analysis:
The disclosure identifies a mismatch between NHS AI deployment and staff competence, training, AI literacy, patient-data handling rules, prompt safety, output verification duties, audit-log consequences, and disciplinary-use boundaries.
The concern is intensified where staff receive AI tools while public messaging warns of dismissal or prison for improper patient-record access.
The disclosure asserts that staff cannot understand their responsibilities if the AI system’s data access, logging, telemetry, retention, support-access, output-reliance, and disciplinary-use consequences are unclear.
The disclosure therefore identifies that AI training, role-specific guidance, patient-data input rules, verification duties, protected-disclosure routes, and audit-log explanation must precede exposure and liability.
VI.6 Caldicott Principle 6 — Comply With the Law
Source:
Caldicott Principles — Principle 6, comply with the law.
Material source: GOV.UK — The Caldicott Principles.
URL: https://www.gov.uk/government/publications/the-caldicott-principles
Verbatim / principle:
“Every use of confidential information must be lawful.”
Analysis:
The disclosure identifies that NHS AI processing engages overlapping legal duties, including common law confidentiality, human rights, equality law, data protection, clinical safety, employment law, public law, evidential fairness, and international privacy principles.
The disclosure asserts that lawfulness cannot be established merely by pointing to NHS operational purpose, public task, service management, or UK storage.
The relevant legal question is whether the complete AI pathway is lawful:
patient input → system execution → AI output → human review → record consequence → audit trail → vendor chain → legal accountability → exit route.
The disclosure therefore identifies that every AI use of confidential information must be assessed across purpose, necessity, proportionality, consent or transparency, security, accuracy, equality, accountability, redress, and preservation.
VI.7 Caldicott Principle 7 — Duty to Share Can Be as Important as Duty to Protect
Source:
Caldicott Principles — Principle 7, duty to share can be as important as duty to protect.
Material source: GOV.UK — The Caldicott Principles.
URL: https://www.gov.uk/government/publications/the-caldicott-principles
Verbatim / principle:
“The duty to share information for individual care is as important as the duty to protect patient confidentiality.”
Analysis:
The disclosure does not assert that NHS data should never be shared for care.
The disclosure accepts that information sharing may be necessary for individual care, operational continuity, and safe treatment.
The concern is that the duty to share for care must not be converted into an open-ended justification for opaque AI processing, vendor access, telemetry extraction, support-access exposure, model monitoring, or externally administered processing environments beyond what is necessary and proportionate for the patient-care purpose.
The disclosure therefore identifies the distinction between lawful care sharing and excessive AI-mediated processing.
The duty to share cannot extinguish the duty to protect.
VI.8 Caldicott Principle 8 — Inform Patients and Service Users About How Their Confidential Information Is Used
Source:
Caldicott Principles — Principle 8, inform patients and service users about how their confidential information is used.
Material source: GOV.UK — The Caldicott Principles.
URL: https://www.gov.uk/government/publications/the-caldicott-principles
Verbatim / principle:
“Inform patients and service users about how their confidential information is used.”
Analysis:
The disclosure identifies that patients must be clearly informed where AI systems process their confidential information.
This includes AI triage, NHS App routing, ambient voice capture, AI scribing, clinical summarisation, automated booking, staff-facing AI tools processing patient-adjacent data, logs, telemetry, support access, model monitoring, and vendor processing.
The disclosure asserts that patients cannot be said to understand how their confidential information is used if the public record does not visibly explain the AI execution pathway, vendor chain, processing location, outputs generated, retention rules, correction route, objection route, and equivalent non-AI access route.
The disclosure therefore identifies patient information as a central safeguard, not a peripheral privacy notice.
VII. UK GDPR and Data Protection Act 2018 — Statutory Data Protection Layer
VII.1 UK GDPR Article 5 — Core Processing Principles
Source:
UK GDPR, Article 5 — Principles relating to processing of personal data.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Article 5, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/article/5
Verbatim / principle:
“Personal data shall be processed lawfully, fairly and in a transparent manner in relation to the data subject.”“Personal data shall be collected for specified, explicit and legitimate purposes.”
“Personal data shall be adequate, relevant and limited to what is necessary.”
“Personal data shall be accurate and, where necessary, kept up to date.”
“Personal data shall be processed in a manner that ensures appropriate security of the personal data.”
“The controller shall be responsible for, and be able to demonstrate compliance with, paragraph 1.”
Analysis:
The disclosure identifies that NHS AI systems processing patient symptom data, patient voice data, clinical notes, triage answers, ambient voice transcripts, staff prompts, AI-generated summaries, audit logs, telemetry, model-monitoring records, and support-access records engage the Article 5 threshold.
The disclosure asserts that AI-mediated healthcare processing cannot be assessed only by reference to general NHS operational purpose or storage location.
The relevant concern is whether the patient or worker can reasonably understand what AI system is processing the data, what data enters the system, where execution and inference occur, who controls the processing chain, which vendors and sub-processors are involved, whether outputs may affect care access or records, and whether the data subject has a meaningful route to access, challenge, correct, object, or refuse.
The disclosure therefore identifies Article 5 as the statutory data-protection foundation for testing NHS AI lawfulness, fairness, transparency, purpose limitation, minimisation, accuracy, security, and accountability across the complete AI chain.
VII.2 UK GDPR Article 6 — Lawful Basis for Processing
Source:
UK GDPR, Article 6 — Lawfulness of processing.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Article 6, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/article/6
Verbatim / principle:
“Processing shall be lawful only if and to the extent that at least one of the following applies.”“Processing is necessary for the performance of a task carried out in the public interest or in the exercise of official authority vested in the controller.”
Analysis:
The disclosure identifies that NHS bodies may rely upon public-task processing for healthcare delivery, administration, safety, and service management.
The disclosure contests whether that lawful basis automatically extends to every AI-mediated processing layer.
The concern applies to AI triage, ambient voice capture, AI transcription, summarisation, staff-facing AI tools, prompt processing, telemetry, support access, model monitoring, product improvement, audit profiling, and AI-derived evidential use.
The statutory question is not whether healthcare is a public task.
The statutory question is whether each AI-processing layer is necessary for that public task and remains proportionate, transparent, accountable, and within the patient’s reasonable expectation of NHS medical processing.
VII.3 UK GDPR Article 9 — Special Category Health Data
Source:
UK GDPR, Article 9 — Processing of special categories of personal data.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Article 9, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/article/9
Verbatim / principle:
“Processing of personal data revealing racial or ethnic origin, political opinions, religious or philosophical beliefs… genetic data, biometric data… data concerning health… shall be prohibited.”
Processing may be permitted where necessary for:
“medical diagnosis, the provision of health or social care or treatment or the management of health or social care systems and services.”
Analysis:
The disclosure identifies NHS patient information as special category data.
The relevant data includes symptoms, diagnosis, medication, disability information, mental-health disclosure, safeguarding material, appointment behaviour, consultation speech, clinical notes, triage answers, ambient voice transcripts, AI-generated summaries, and inferred health information.
The disclosure further identifies that AI systems may generate special category meaning indirectly through routing outputs, risk flags, urgency classifications, prompts, logs, telemetry, model-monitoring records, and staff audit trails.
The Article 9 concern is that the healthcare exception cannot become an unlimited gateway for opaque AI processing, SaaS execution, telemetry capture, vendor support access, model improvement, or secondary evidential use.
The disclosure therefore identifies that each special-category AI-processing layer must be justified by necessity, medical purpose, safeguards, confidentiality, transparency, and proportionality.
VII.4 UK GDPR Articles 13–14 — Transparency and Information Duties
Source:
UK GDPR, Articles 13 and 14 — Information to be provided where personal data is collected from the data subject or obtained otherwise.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Articles 13 and 14, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/article/13
URL: https://www.legislation.gov.uk/eur/2016/679/article/14
Verbatim / principle:
“Where personal data relating to a data subject are collected from the data subject, the controller shall, at the time when personal data are obtained, provide the data subject with… information.”“Where personal data have not been obtained from the data subject, the controller shall provide the data subject with… information.”
Analysis:
The disclosure identifies that Articles 13 and 14 are engaged where patients provide symptoms, voice data, triage answers, appointment requests, consultation information, or clinical material into AI-mediated routes.
They are also engaged where AI systems generate or infer personal data not directly supplied by the patient or worker.
This may include AI-generated summaries, triage classifications, urgency scores, routing outputs, staff usage records, telemetry, model-monitoring signals, audit logs, support records, inferred risk categories, and behavioural access patterns.
The disclosure asserts that patients and workers must be informed of AI processing at the point where the processing occurs, not merely through remote generic privacy notices.
The Article 13–14 concern is that transparency must cover the AI system, purpose, vendor chain, data categories, outputs generated, retention, logging, telemetry, model monitoring, support access, objection route, access route, and correction route.
VII.5 UK GDPR Article 15 — Right of Access
Source:
UK GDPR, Article 15 — Right of access by the data subject.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Article 15, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/article/15
Verbatim / principle:
“The data subject shall have the right to obtain from the controller confirmation as to whether or not personal data concerning him or her are being processed.”
Analysis:
The disclosure identifies that patients and workers must be able to access AI-derived personal data concerning them.
For patients, this may include symptom inputs, adaptive questions, triage outputs, routing decisions, ambient voice transcripts, AI-generated summaries, draft notes, final clinical notes, correction records, objection records, and relevant logs.
For workers, this may include prompts, outputs, usage records, Copilot logs, audit trails, access histories, telemetry linked to user identity, investigation material, and AI-derived performance or disciplinary records.
The Article 15 concern is that access rights are undermined where AI records are distributed across NHS systems, vendors, cloud providers, telemetry systems, model-monitoring services, support platforms, and local records.
The disclosure therefore identifies that NHS AI systems must make AI-derived records discoverable, retrievable, intelligible, and attributable.
VII.6 UK GDPR Article 16 — Right to Rectification
Source:
UK GDPR, Article 16 — Right to rectification.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Article 16, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/article/16
Verbatim / principle:
“The data subject shall have the right to obtain from the controller without undue delay the rectification of inaccurate personal data concerning him or her.”
Analysis:
The disclosure identifies that AI systems may create inaccurate personal data through mistranscription, hallucination, omission, summarisation error, routing error, accent misrecognition, classification error, or incorrect inference.
This applies to AI triage outputs, ambient voice transcripts, AI-generated clinical summaries, staff audit records, access logs, model-generated classifications, support records, and AI-derived evidence.
The disclosure asserts that rectification must follow the error wherever it persists.
If an ambient voice system mistranscribes a consultation, the error may exist in the transcript, draft summary, final clinical record, audit trail, support ticket, and model-monitoring data.
The Article 16 concern is that correcting only the final visible record may leave inaccurate AI-derived data active in hidden processing layers.
VII.7 UK GDPR Articles 17–18 — Erasure and Restriction of Processing
Source:
UK GDPR, Articles 17 and 18 — Right to erasure and right to restriction of processing.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Articles 17 and 18, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/article/17
URL: https://www.legislation.gov.uk/eur/2016/679/article/18
Verbatim / principle:
“The data subject shall have the right to obtain from the controller the erasure of personal data concerning him or her without undue delay.”“The data subject shall have the right to obtain from the controller restriction of processing.”
Analysis:
The disclosure identifies that NHS AI systems may retain patient or worker data in multiple layers beyond the final visible record.
Those layers may include prompts, transcripts, generated summaries, draft records, logs, telemetry, model-monitoring records, support tickets, debugging records, backups, audit trails, and improvement datasets.
The disclosure asserts that erasure and restriction rights become difficult to exercise where AI-derived data is replicated across vendors, processors, sub-processors, telemetry systems, support platforms, and local NHS environments.
The Article 17–18 concern is that NHS AI deployment must clarify which AI-derived records can be erased, which must be retained, why they are retained, where they are retained, how restriction is applied, and how disputed AI-derived records are isolated pending resolution.
VII.8 UK GDPR Article 21 — Right to Object
Source:
UK GDPR, Article 21 — Right to object.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Article 21, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/article/21
Verbatim / principle:
“The data subject shall have the right to object, on grounds relating to his or her particular situation, at any time to processing of personal data concerning him or her.”
Analysis:
The disclosure identifies that patients may have particular reasons to object to AI-mediated processing.
Those reasons may include medical vulnerability, safeguarding concern, domestic abuse risk, mental-health sensitivity, disability, mistrust of voice capture, shared-device risk, litigation context, whistleblowing context, confidentiality concern, or prior data-governance harm.
Workers may also object where staff-facing AI processing creates prompt retention, usage records, telemetry, audit logs, disciplinary exposure, equality risk, or protected-disclosure risk.
The Article 21 concern is that objection rights are not meaningful if refusal of AI produces poorer access, delayed care, degraded service, employment disadvantage, or absence of an equivalent human route.
The disclosure therefore identifies that NHS AI deployment must preserve practical, accessible, equivalent objection and fallback routes.
VII.9 UK GDPR Article 22 — Automated Decision-Making and Profiling
Source:
UK GDPR, Article 22 — Automated individual decision-making, including profiling.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Article 22, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/article/22
Verbatim / principle:
“The data subject shall have the right not to be subject to a decision based solely on automated processing, including profiling, which produces legal effects concerning him or her or similarly significantly affects him or her.”
Analysis:
The disclosure identifies that AI triage, automated routing, staff audit profiling, AI-generated disciplinary material, risk scoring, and algorithmic access pathways may materially affect patients or workers even where systems are described as support tools.
The concern is practical effect.
If AI triage influences whether a patient is routed to GP, pharmacy, A&E, self-care, urgent review, delayed appointment, or digital-only advice, the patient may be significantly affected.
If AI audit logs or staff AI-use records influence disciplinary action, dismissal, capability assessment, tribunal evidence, or professional reputation, the worker may be significantly affected.
The Article 22 concern is that NHS bodies must not avoid scrutiny by labelling AI outputs as advisory while those outputs materially shape access, care, records, employment risk, or evidential reliance.
VII.10 UK GDPR Article 25 — Data Protection by Design and Default
Source:
UK GDPR, Article 25 — Data protection by design and by default.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Article 25, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/article/25
Verbatim / principle:
The controller shall implement “appropriate technical and organisational measures” designed to implement data-protection principles and protect the rights of data subjects.
Analysis:
The disclosure identifies that NHS AI safeguards must be built into the system before deployment.
The relevant measures include data minimisation, role-based access, prompt controls, output labelling, retention limits, telemetry minimisation, support-access controls, audit visibility, patient objection route, staff access rights, correction routes, human review, and equivalent non-AI routes.
The disclosure asserts that safeguards cannot be retrofitted after dependency forms, logs accumulate, workflows adapt, patients are routed, staff are audited, and AI-generated records enter clinical or employment systems.
The Article 25 concern is that NHS AI must be privacy-protective by architecture, not by later explanation.
VII.11 UK GDPR Article 28 — Processor and Sub-Processor Controls
Source:
UK GDPR, Article 28 — Processor.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Article 28, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/article/28
Verbatim / principle:
“Where processing is to be carried out on behalf of a controller, the controller shall use only processors providing sufficient guarantees.”
Analysis:
The disclosure identifies that NHS AI deployment may involve multiple processors and sub-processors, including SaaS vendors, cloud providers, AI model providers, speech-to-text providers, telemetry providers, support providers, analytics services, backup providers, and security monitoring providers.
The Article 28 concern is that the public cannot assess lawful processing unless the processor and sub-processor chain is visible.
The disclosure further identifies that processor guarantees must cover not only storage, but execution, inference, logging, support access, telemetry, model monitoring, data retention, breach handling, deletion, audit, and transfer safeguards.
The disclosure therefore identifies that NHS AI cannot be assessed by naming only the front-end product. The full processing chain must be disclosed and governed.
VII.12 UK GDPR Article 30 — Records of Processing Activities
Source:
UK GDPR, Article 30 — Records of processing activities.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Article 30, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/article/30
Verbatim / principle:
“Each controller and, where applicable, the controller’s representative, shall maintain a record of processing activities under its responsibility.”
Analysis:
The disclosure identifies that NHS AI systems require records of processing that describe the actual processing activities taking place.
Those records must cover AI triage, ambient voice, AI scribing, staff-facing AI tools, prompts, outputs, logs, telemetry, vendor support, model monitoring, data flows, recipients, retention periods, security measures, and international transfers where relevant.
The Article 30 concern is that records of processing must reflect the AI execution chain, not merely generic categories of digital administration.
The disclosure therefore identifies that NHS bodies must be able to produce records showing what personal data is processed, for what purpose, by whom, where, for how long, and under what safeguards.
VII.13 UK GDPR Article 32 — Security of Processing
Source:
UK GDPR, Article 32 — Security of processing.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Article 32, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/article/32
Verbatim / principle:
The controller and processor shall implement “appropriate technical and organisational measures to ensure a level of security appropriate to the risk.”
Analysis:
The disclosure identifies that NHS AI security must address the full risk environment.
This includes confidentiality of patient data, integrity of AI outputs, availability of systems, resilience of processing, audit-log security, prompt security, transcript security, telemetry security, support-access controls, vendor-access controls, backup security, and recovery from incident or service failure.
The Article 32 concern is that healthcare AI risk is not limited to unauthorised access.
Authorised processing itself can create exposure through prompts, outputs, transcripts, logs, telemetry, support records, model-monitoring records, and audit trails.
The disclosure therefore identifies that AI cybersecurity must protect system exhaust as well as the clinical database.
VII.14 UK GDPR Article 35 — Data Protection Impact Assessment
Source:
UK GDPR, Article 35 — Data protection impact assessment.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Article 35, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/article/35
Verbatim / principle:
“Where a type of processing… is likely to result in a high risk to the rights and freedoms of natural persons, the controller shall… carry out an assessment of the impact of the envisaged processing operations.”
Analysis:
The disclosure identifies NHS AI deployment as high-risk processing because it involves special-category health data, vulnerable data subjects, new technology, large-scale processing, possible automated or semi-automated routing, voice capture, staff audit exposure, cloud processing, vendor chains, and patient-access consequences.
The Article 35 concern is that DPIAs must visibly address AI triage, ambient voice, AI scribing, Copilot-style workflow tools, execution location, telemetry, support access, model monitoring, re-identification risk, cross-border processing, equality impact, staff audit exposure, patient objection routes, and AI-derived evidence.
The disclosure therefore identifies DPIA visibility as central to lawful NHS AI deployment.
VII.15 UK GDPR Articles 44–49 — International Transfers
Source:
UK GDPR, Articles 44–49 — Transfers of personal data to third countries or international organisations.
Material source: legislation.gov.uk — Regulation (EU) 2016/679, Chapter V, Articles 44–49, retained UK GDPR.
URL: https://www.legislation.gov.uk/eur/2016/679/chapter/V
Verbatim / principle:
“Any transfer of personal data… to a third country or to an international organisation shall take place only if… the conditions laid down in this Chapter are complied with.”
Analysis:
The disclosure identifies that international-transfer risk cannot be assessed only by asking where the primary database is stored.
AI processing may involve execution, inference, logs, telemetry, support access, model monitoring, backups, disaster recovery, analytics, security tooling, and sub-processor access across different jurisdictions.
The disclosure further identifies that foreign-controlled cloud, SaaS, AI model, support, and telemetry providers may create legal and practical sovereignty questions even where UK storage is asserted.
The Articles 44–49 concern is therefore whether any part of the AI processing chain involves transfer, remote access, support access, cross-border processing, or foreign legal control requiring safeguards.
The disclosure position remains:
The breach is not where the data rests. The breach is where the data acts.
VII.16 Data Protection Act 2018 — Domestic Statutory Supplement to UK GDPR
Source:
Data Protection Act 2018.
Material source: legislation.gov.uk — Data Protection Act 2018.
URL: https://www.legislation.gov.uk/ukpga/2018/12/contents
Verbatim / principle:
“An Act to make provision for the regulation of the processing of information relating to individuals.”
Analysis:
The disclosure identifies the Data Protection Act 2018 as the domestic statutory layer sitting alongside UK GDPR.
The disclosure asserts that NHS AI deployment cannot be treated as general digital administration where processing involves patient medical data, symptom data, voice data, clinical notes, staff prompts, audit logs, telemetry, AI-generated summaries, triage outputs, and derived or inferred personal data.
The statutory concern is that NHS AI systems may process personal data across multiple layers, including direct patient input, clinical data, special category health data, staff-use data, AI-generated records, logs, telemetry, support records, model-monitoring records, and re-identification-capable datasets.
The disclosure therefore identifies that the Data Protection Act 2018 reinforces the requirement for lawful, necessary, proportionate, secure, accountable, rights-compatible processing across the complete AI chain.
VII.17 Data Protection Act 2018 — Section 10 and Schedule 1, Special Category Processing Conditions
Source:
Data Protection Act 2018, Section 10 and Schedule 1.
Material source: legislation.gov.uk — Data Protection Act 2018, Section 10 and Schedule 1.
URL: https://www.legislation.gov.uk/ukpga/2018/12/section/10
URL: https://www.legislation.gov.uk/ukpga/2018/12/schedule/1
Verbatim / principle:
“Subsections (2) and (3) make provision about the processing of special categories of personal data.”
Schedule 1 provides conditions for processing special category personal data, including health or social care purposes and public health purposes.
Analysis:
The disclosure identifies that NHS AI deployment engages special category processing because the data includes health data, disability information, medication information, clinical notes, symptoms, diagnosis, mental-health disclosures, safeguarding material, voice-derived consultation data, triage answers, and medical-record content.
The disclosure further identifies that AI systems may generate or infer special category meaning even where the original input appears administrative.
Appointment behaviour may reveal health status. Triage answers may reveal symptoms. Voice transcripts may reveal disability, distress, impairment, accent, language, or mental-health condition. AI summaries may reveal diagnosis, treatment, medication, vulnerability, or safeguarding context. Telemetry may reveal clinical pathway. Staff prompts may include patient medical context.
The Section 10 and Schedule 1 concern is that special category health data requires heightened statutory safeguards.
The disclosure therefore identifies that NHS AI processing must be assessed as special-category processing not only at the clinical-record layer, but also at the AI-output, log, telemetry, support-access, model-monitoring, and staff-audit layers.
VII.18 Data Protection Act 2018 — Schedule 1, Health or Social Care Purposes
Source:
Data Protection Act 2018, Schedule 1, Part 1, paragraph 2.
Material source: legislation.gov.uk — Data Protection Act 2018, Schedule 1, Part 1, paragraph 2.
URL: https://www.legislation.gov.uk/ukpga/2018/12/schedule/1/paragraph/2
Verbatim / principle:
Processing is permitted where it is necessary for health or social care purposes and is carried out by, or under the responsibility of, a health professional or another person who owes a duty of confidentiality.
Analysis:
The disclosure recognises that health and social care purposes may justify special category processing where the statutory conditions are properly met.
The disclosure contests whether all NHS AI processing layers remain necessary for health or social care purposes.
The concern applies to AI triage, ambient voice capture, AI transcription, AI summarisation, Copilot-style workflow processing, telemetry, model monitoring, support access, product improvement, staff audit profiling, disciplinary-use records, and AI-derived evidential material.
The disclosure therefore identifies that “health or social care purposes” cannot be treated as unlimited statutory cover for every AI, SaaS, cloud, telemetry, vendor, analytics, support, and model-monitoring pathway.
The statutory question remains which processing is necessary for care, and which processing is secondary system exhaust.
VII.19 Data Protection Act 2018 — Schedule 1, Public Health
Source:
Data Protection Act 2018, Schedule 1, Part 1, paragraph 3.
Material source: legislation.gov.uk — Data Protection Act 2018, Schedule 1, Part 1, paragraph 3.
URL: https://www.legislation.gov.uk/ukpga/2018/12/schedule/1/paragraph/3
Verbatim / principle:
Processing is permitted where it is necessary for reasons of public interest in the area of public health.
Analysis:
The disclosure recognises that public health processing may be lawful where properly justified.
The disclosure contests whether AI deployment for productivity, triage efficiency, administrative automation, staff workflow, ambient documentation, or operational dashboards can be treated as public-health processing without a visible necessity and proportionality assessment.
The concern is that broad public-health language may obscure specific AI-processing activities.
The disclosure identifies that public health does not automatically justify opaque model execution, undisclosed sub-processors, broad telemetry, support-access exposure, model improvement use, re-identification-capable analytics, or patient-data processing beyond direct care necessity.
The disclosure therefore identifies that any reliance on public health must be mapped to the exact AI processing purpose and safeguarded accordingly.
VII.20 Data Protection Act 2018 — Schedule 1, Research Purposes
Source:
Data Protection Act 2018, Schedule 1 — research-related processing conditions and safeguards.
Material source: legislation.gov.uk — Data Protection Act 2018, Schedule 1.
URL: https://www.legislation.gov.uk/ukpga/2018/12/schedule/1
Verbatim / principle:
Schedule 1 makes provision for special category processing conditions and safeguards, including processing connected with research and public-interest purposes where applicable conditions are met.
Analysis:
The disclosure identifies that NHS AI systems may blur the boundary between care delivery, service management, model evaluation, product improvement, and research-like secondary processing.
Where patient data, triage outputs, clinician overrides, ambient voice transcripts, correction records, red-flag misses, model-monitoring data, or performance telemetry are used to improve AI products or evaluate models, the processing may move toward research, development, evaluation, or secondary-use territory.
The disclosure asserts that this boundary must be explicit.
Patients may provide data for care.
That does not automatically mean their data may be used for AI model improvement, product optimisation, commercial refinement, training-signal extraction, or performance analytics without clear lawful basis and safeguards.
The statutory concern is therefore whether AI improvement activity is being treated as invisible operational processing rather than separately governed secondary processing.
VII.21 Data Protection Act 2018, Section 170 — Unlawful Obtaining, Disclosure, or Retention of Personal Data
Source:
Data Protection Act 2018, Section 170.
Material source: legislation.gov.uk — Data Protection Act 2018, Section 170.
URL: https://www.legislation.gov.uk/ukpga/2018/12/section/170
Verbatim / principle:
“It is an offence for a person knowingly or recklessly—
to obtain or disclose personal data without the consent of the controller.”
Analysis:
The disclosure identifies that NHS AI systems expand the number of routes by which personal data may be obtained, disclosed, retained, accessed, copied, logged, exported, or reproduced.
The concern is not limited to deliberate criminal misuse.
The disclosure identifies exposure risk through support tickets, screenshots, prompts, copied clinical text, debugging records, transcripts, AI summaries, vendor logs, telemetry, audit extracts, and model-monitoring records.
The Section 170 concern is that personal data may be handled outside properly authorised boundaries where AI systems generate secondary records that staff, vendors, support personnel, or sub-processors can access or retain.
The disclosure further identifies that staff cannot be threatened with severe consequences for record misuse while the institution fails to disclose the authorised processing chain, support-access controls, vendor boundaries, and audit rules.
VII.22 Data Protection Act 2018, Section 171 — Re-Identification of De-Identified Personal Data
Source:
Data Protection Act 2018, Section 171.
Material source: legislation.gov.uk — Data Protection Act 2018, Section 171.
URL: https://www.legislation.gov.uk/ukpga/2018/12/section/171
Verbatim / principle:
“It is an offence for a person knowingly or recklessly to re-identify information that is de-identified personal data without the consent of the controller.”
Analysis:
The disclosure identifies re-identification risk as central to NHS AI deployment.
The concern is that AI systems may process data that appears pseudonymised, de-identified, anonymised, masked, aggregated, or technical, while still retaining identity through pattern.
Identity may arise through symptom sequence, rare condition, appointment timing, GP practice, postcode area, medication pattern, voice markers, accent, clinical pathway, staff-user behaviour, audit logs, telemetry, prompts, and generated summaries.
The disclosure asserts that re-identification is not a remote theoretical issue where AI systems are designed to detect correlations across large datasets.
The Section 171 concern is therefore that pseudonymisation, de-identification, or name removal cannot be treated as final protection unless AI-era linkage, inference, and pattern-correlation risks are assessed.
Core position:
In AI systems, the pattern is the person.
VII.23 Data Protection Act 2018, Section 173 — Alteration of Personal Data to Prevent Disclosure
Source:
Data Protection Act 2018, Section 173.
Material source: legislation.gov.uk — Data Protection Act 2018, Section 173.
URL: https://www.legislation.gov.uk/ukpga/2018/12/section/173
Verbatim / principle:
It is an offence to alter, deface, block, erase, destroy or conceal information with the intention of preventing disclosure of information a person would have been entitled to receive.
Analysis:
The disclosure identifies that AI systems create multiple layers of records that may be required in subject access, tribunal, disciplinary, clinical complaint, negligence, equality, whistleblowing, regulatory, or public-interest contexts.
Those records may include prompts, AI outputs, draft summaries, final summaries, ambient transcripts, raw audio status, triage outputs, model version, source documents, edit history, correction history, audit logs, telemetry, support tickets, and model-monitoring records.
The Section 173 concern is that AI-derived records must not be deleted, obscured, overwritten, normalised, concealed, or removed once disclosure rights, complaint rights, patient-record rights, tribunal relevance, or procedural reliance arise.
The disclosure therefore identifies the need for preservation rules governing AI-derived material, especially where it may later be required for data subject rights, protected disclosure, clinical safety review, patient-record correction, disciplinary evidence, or tribunal evidence.
VII.24 UK GDPR Article 5(2) and Article 35 — Accountability Principle and Undetermined Extraterritorial Engagement
Source: UK GDPR Article 5(2) — Accountability principle; UK GDPR Article 35 — Data Protection Impact Assessment; UK GDPR Articles 44–49 and EU AI Act Article 2(1)(c) — international transfer and extraterritorial output-use triggers. Material source: legislation.gov.uk — UK GDPR, Article 5(2) and Article 35. URL: https://www.legislation.gov.uk/eur/2016/679/article/5 URL: https://www.legislation.gov.uk/eur/2016/679/article/35
Verbatim / principle: "The controller shall be responsible for, and be able to demonstrate compliance with, paragraph 1 ('accountability')."
Analysis: The disclosure does not assert that the EU AI Act, or the international-transfer provisions of UK GDPR, are definitively engaged by NHS AI deployment.
The disclosure asserts that this question cannot presently be answered from the public record, and that the inability to answer it is itself the breach.
Whether AI system output is used within the European Union, whether any deployer or sub-processor is established there, whether telemetry, model-monitoring, or support-access data is processed there, and whether any cross-border transfer safeguard under Articles 44–49 is engaged, all depend on facts that have not been published: the execution map, the sub-processor chain, and the DPIA required under Article 35.
Under Article 5(2), the burden of demonstrating compliance including the jurisdictional footprint of processing rests with the controller, not with the patient, worker, or public.
The disclosure therefore identifies that the possible engagement of the EU AI Act, GDPR Chapter V transfer safeguards, or equivalent extraterritorial obligations remains undetermined pending disclosure, and that this undetermined status is not a neutral gap but an active accountability failure, since the controller not the public carries the evidential burden to resolve it.
VIII. Clinical Safety, Health IT, Medical Device, and Healthcare Records Governance Layer
VIII.1 Health and Social Care Act 2012 — Information Standards and Clinical Safety Governance
Source:
Health and Social Care Act 2012 — statutory basis for health service information standards and NHS information governance functions.
Material source: legislation.gov.uk — Health and Social Care Act 2012.
URL: https://www.legislation.gov.uk/ukpga/2012/7/contents
Verbatim / principle:
The Act provides statutory powers and governance structures concerning health service functions, information standards, and health service administration.
Analysis:
The disclosure identifies that NHS AI triage, ambient voice technology, AI scribing, automated routing, clinical summarisation, workflow automation, and patient-record formation engage clinical safety governance because they may affect patient access, clinical documentation, urgency classification, future care, and system-level patient safety.
The disclosure asserts that AI systems cannot be treated as ordinary administrative software where they influence clinical pathways, clinical records, staff workflow, patient routing, or patient safety.
The statutory concern is that health IT systems affecting care must be clinically safe, risk assessed, documented, monitored, and governed before deployment.
The disclosure therefore identifies that NHS AI systems require visible clinical safety assurance, including hazard identification, risk controls, residual-risk approval, clinical safety responsibility, and incident-monitoring routes.
VIII.2 DCB0129 — Clinical Risk Management in Manufacture of Health IT Systems
Source:
DCB0129 — Clinical Risk Management: its Application in the Manufacture of Health IT Systems.
Material source: NHS Digital / NHS England — DCB0129 clinical safety standard.
URL: https://digital.nhs.uk/data-and-information/information-standards/governance/latest-activity/standards-and-collections/dcb0129-clinical-risk-management-its-application-in-the-manufacture-of-health-it-systems
Verbatim / principle:
DCB0129 is a clinical risk management standard concerning the manufacture of health IT systems.
Analysis:
The disclosure identifies that vendors supplying AI triage, ambient voice, AI scribing, clinical summarisation, automated booking, or patient-access software may be manufacturing health IT systems capable of affecting clinical safety.
The disclosure asserts that such systems require manufacturer-side clinical risk management, including identification of hazards, foreseeable harms, risk controls, safety documentation, clinical safety case production, and residual-risk management.
The concern applies where an AI system may misroute a patient, under-triage symptoms, mistranscribe clinical speech, omit red flags, hallucinate a summary, create an inaccurate clinical note, or generate output relied upon by NHS staff.
The disclosure therefore identifies that DCB0129 evidence must be visible where AI products are being placed into patient-facing, staff-facing, triage, or clinical-documentation pathways.
VIII.3 DCB0160 — Clinical Risk Management in Deployment and Use of Health IT Systems
Source:
DCB0160 — Clinical Risk Management: its Application in the Deployment and Use of Health IT Systems.
Material source: NHS Digital / NHS England — DCB0160 clinical safety standard.
URL: https://digital.nhs.uk/data-and-information/information-standards/information-standards-and-data-collections-including-extractions/publications-and-notifications/standards-and-collections/dcb0160-clinical-risk-management-its-application-in-the-deployment-and-use-of-health-it-systems
Verbatim / principle:
DCB0160 is a clinical risk management standard concerning the deployment and use of health IT systems.
Analysis:
The disclosure identifies that NHS England, Integrated Care Boards, NHS trusts, GP practices, and deploying organisations must assess clinical risk when AI systems are deployed into live healthcare pathways.
The disclosure asserts that deployment risk is separate from vendor design risk.
Even where a supplier claims its product is safe, the deploying NHS organisation must assess how the system operates in its own environment, patient population, staff workflow, data infrastructure, equality context, language profile, accessibility profile, and clinical escalation pathway.
The concern applies to NHS App AI triage, GP automated booking, ambient voice products, AI-generated clinical notes, staff-facing AI tools processing patient-adjacent material, and AI outputs entering records or care routes.
The disclosure therefore identifies that DCB0160 deployment assurance must be visible before national or local reliance forms.
VIII.4 Digital Clinical Safety Assurance — Hazard Logs and Clinical Safety Cases
Source:
NHS England — Digital Clinical Safety Assurance.
Material source: NHS England — Digital clinical safety assurance.
URL: https://www.england.nhs.uk/long-read/digital-clinical-safety-assurance/
Verbatim / principle:
A hazard log records hazards considered attributable to the product, the potential clinical impact, mitigations, controls, and final assessment of risk.
Analysis:
The disclosure identifies that NHS AI systems require visible hazard analysis because AI tools may generate clinical, operational, evidential, and record-formation risk.
The relevant hazards include under-triage, misrouting, hallucinated summaries, mistranscription, missed red flags, accent error, disability-related access failure, automation bias, staff overreliance, unclear override rules, incorrect audit interpretation, and inability to correct AI-derived records.
The disclosure asserts that a clinical safety case must not merely state that a tool is safe.
It must show the hazards considered, the severity of potential harm, the mitigation controls, the residual risk, the accountable clinical safety officer, and the monitoring route after deployment.
The disclosure therefore identifies hazard logs and clinical safety cases as required evidence for assessing whether NHS AI deployment is safe in practice.
VIII.5 Digital Technology Assessment Criteria — Clinical Safety, Data Protection, Security, Interoperability, Usability, and Accessibility
Source:
Digital Technology Assessment Criteria for Health and Social Care.
Material source: NHS England Transformation Directorate — DTAC.
URL: https://transform.england.nhs.uk/key-tools-and-info/digital-technology-assessment-criteria-dtac/
Verbatim / principle:
DTAC assesses digital health technologies across clinical safety, data protection, technical security, interoperability, usability, and accessibility.
Analysis:
The disclosure identifies that NHS AI systems must be assessed as digital health technologies where they affect patient access, clinical documentation, workflow, records, or care delivery.
The disclosure asserts that AI deployment must not be justified only through productivity claims, queue reduction, staff-time saving, administrative convenience, or national digital-transformation language.
The DTAC concern is that safe NHS AI deployment requires assessment across the full stack: clinical safety, data protection, technical security, interoperability, usability, accessibility, equality of access, human fallback, and safe integration with clinical systems.
The disclosure therefore identifies DTAC as engaged where AI tools are being embedded into NHS App routing, GP access, ambient voice, AI scribing, triage, or staff-facing workflow environments.
VIII.6 UK Medical Device Regulations 2002 — Software With a Medical Purpose
Source:
Medical Devices Regulations 2002.
Material source: legislation.gov.uk — Medical Devices Regulations 2002.
URL: https://www.legislation.gov.uk/uksi/2002/618/contents
Verbatim / principle:
Medical device regulation may apply to software where the intended purpose brings it within regulated medical device functions.
Analysis:
The disclosure identifies that NHS AI tools may require medical-device assessment where their outputs influence diagnosis, symptom assessment, triage priority, clinical routing, treatment advice, monitoring, prediction, prognosis, or patient management.
The concern is particularly engaged by AI triage, symptom checkers, risk classification, urgency classification, AI-generated clinical summaries, and systems producing outputs capable of influencing care.
The disclosure does not assert that every NHS AI product is automatically a medical device.
The disclosure asserts that the public record must show whether each AI system has been assessed for medical-device status and, where excluded, the reason for exclusion.
The disclosure therefore identifies regulatory classification as a required disclosure point before AI systems are relied upon in healthcare pathways.
VIII.7 MHRA Software and AI as a Medical Device Guidance
Source:
MHRA — Software and Artificial Intelligence as a Medical Device.
Material source: GOV.UK — Software and artificial intelligence (AI) as a medical device.
URL: https://www.gov.uk/government/publications/software-and-artificial-intelligence-ai-as-a-medical-device/software-and-artificial-intelligence-ai-as-a-medical-device
Verbatim / principle:
Software, including AI, may be regulated as a medical device or in vitro diagnostic medical device where it meets the relevant regulatory criteria.
Analysis:
The disclosure identifies that AI systems used in NHS care may blur boundaries between administration, decision support, documentation, and clinical function.
The concern applies where a tool is marketed as administrative but practically affects clinical decision-making, patient routing, safety escalation, record formation, or diagnosis-related workflow.
The disclosure asserts that intended purpose and practical effect must both be examined.
If AI output affects clinical access, clinical record accuracy, urgency classification, clinician reliance, patient management, or escalation, then medical-device assessment cannot be bypassed through branding language.
The disclosure therefore identifies the need for MHRA classification evidence, conformity status, post-market monitoring arrangements, incident reporting, and clinical governance routes where AI systems operate near clinical decision points.
VIII.8 NICE Evidence Standards Framework for Digital Health Technologies
Source:
NICE Evidence Standards Framework for Digital Health Technologies.
Material source: NICE — Evidence standards framework for digital health technologies.
URL: https://www.nice.org.uk/corporate/ecd7
Verbatim / principle:
Digital health technologies should be supported by evidence proportionate to their function, risk, and intended use.
Analysis:
The disclosure identifies that NHS AI systems require evidence proportionate to their risk.
The concern is that national deployment cannot rest on headline productivity claims, narrow pilots, self-reported time savings, queue-reduction claims, or vendor assurances where systems affect patients and staff.
The disclosure asserts that evidence should show baseline comparison, task type, user role, error rate, correction time, review time, rework time, clinical safety impact, patient outcome effect, equality impact, accent validation, disability access, and post-deployment monitoring.
The disclosure therefore identifies that AI evidence must be independently auditable before claims of efficiency, safety, access improvement, or workload reduction are used to justify scaling.
VIII.9 Duty of Candour — Openness When Things Go Wrong
Source:
Health and Social Care Act 2008 (Regulated Activities) Regulations 2014, Regulation 20 — Duty of candour.
Material source: legislation.gov.uk — Regulation 20, Duty of candour.
URL: https://www.legislation.gov.uk/uksi/2014/2936/regulation/20
Verbatim / principle:
A registered person must act in an open and transparent way with relevant persons in relation to care and treatment provided.
Analysis:
The disclosure identifies that AI-related harm, near miss, misrouting, under-triage, hallucinated summary, mistranscription, inaccurate patient-record formation, or unsafe automation may engage candour duties.
The disclosure asserts that duty of candour cannot operate properly unless AI involvement is recorded and traceable.
If an AI triage system misroutes a patient, or an ambient voice tool generates an inaccurate clinical note, the patient must be told not only that an error occurred, but whether AI processing contributed to the error.
The concern is that AI involvement may be hidden inside workflow, making incidents appear human-only, administrative-only, or record-only.
The disclosure therefore identifies that AI incident records, source-to-output traceability, model or system version, human review, correction history, and patient notification routes are necessary for candour to be meaningful.
VIII.10 NHS Records Management Code of Practice — AI-Derived Records and Retention
Source:
NHS Records Management Code of Practice.
Material source: NHS England — Records Management Code of Practice.
URL: https://www.nhsx.nhs.uk/information-governance/guidance/records-management-code/
Verbatim / principle:
The Records Management Code of Practice provides guidance on the creation, management, retention, storage, and disposal of health and care records.
Analysis:
The disclosure identifies that AI systems create new classes of records.
Those records may include ambient voice audio status, transcripts, AI-generated summaries, draft clinical notes, final edited notes, triage inputs, triage outputs, prompts, generated text, audit logs, staff AI-use records, telemetry, support tickets, correction histories, model versions, and AI incident records.
The records-management concern is that NHS bodies must define which AI-derived materials form part of the clinical record, which are retained as audit records, which are deleted, which are accessible to patients, and which must be preserved for complaints, litigation, tribunal, clinical safety review, protected disclosure, or subject access.
The disclosure therefore identifies that AI record formation cannot be left to vendor defaults or informal workflow practice.
VIII.11 Professional Duties — Accurate Clinical Records and Confidentiality
Source:
Professional healthcare duties concerning accurate records, confidentiality, and safe care.
Material source: GMC — Good medical practice; NMC Code; HCPC Standards of conduct, performance and ethics.
URL: https://www.gmc-uk.org/professional-standards/good-medical-practice
URL: https://www.nmc.org.uk/standards/code/
URL: https://www.hcpc-uk.org/standards/standards-of-conduct-performance-and-ethics/
Verbatim / principle:
Healthcare professionals are required to keep accurate records, protect patient confidentiality, act within competence, and raise concerns where patient safety is at risk.
Analysis:
The disclosure identifies that AI systems may place clinicians and staff in the position of reviewing, correcting, signing, importing, or relying on AI-generated outputs.
The concern applies to ambient voice summaries, AI scribes, triage outputs, generated correspondence, referral drafts, clinical summaries, AI-assisted administrative records, and staff-facing workflow tools.
The disclosure asserts that professional duties are destabilised where AI introduces errors upstream but the professional becomes the visible endpoint of responsibility.
The relevant risk is:
AI output → staff verification burden → final record → professional liability.
The disclosure therefore identifies that professional record duties require clear AI labelling, source material retention, edit history, correction route, training, safe workload allocation, and protection from unfair attribution where errors originate in the AI system or deployment design.
IX. Employment, Whistleblowing, Staff Safety, and Workplace Protection Layer
IX.1 Employment Rights Act 1996, Section 43B — Qualifying Disclosures
Source:
Employment Rights Act 1996, Section 43B — Disclosures qualifying for protection.
Material source: legislation.gov.uk — Employment Rights Act 1996, Section 43B.
URL: https://www.legislation.gov.uk/ukpga/1996/18/section/43B
Verbatim / principle:
A qualifying disclosure is a disclosure of information which, in the reasonable belief of the worker making the disclosure, is made in the public interest and tends to show one or more forms of wrongdoing, including breach of legal obligation, danger to health and safety, environmental damage, miscarriage of justice, or concealment.
Analysis:
The disclosure identifies that NHS AI deployment may give rise to qualifying disclosure subject matter where workers raise concerns about patient safety, unlawful data processing, confidentiality degradation, unsafe triage, AI hallucination, inaccessible systems, discrimination, inadequate training, misleading productivity claims, or concealment of AI risk.
The disclosure asserts that staff must be able to disclose concerns about AI systems where those systems affect patient access, clinical records, confidential information, staff liability, or public accountability.
The Section 43B concern is that AI governance failures may fall within protected-disclosure territory where the worker reasonably believes the information tends to show legal breach, health and safety danger, or concealment.
The disclosure therefore identifies NHS AI deployment as requiring protected disclosure routes that allow workers to report AI-related risk without retaliation or disciplinary reframing.
IX.2 Employment Rights Act 1996, Section 47B — Protected Disclosure Detriment
Source:
Employment Rights Act 1996, Section 47B — Protected disclosure detriment.
Material source: legislation.gov.uk — Employment Rights Act 1996, Section 47B.
URL: https://www.legislation.gov.uk/ukpga/1996/18/section/47B
Verbatim / principle:
“A worker has the right not to be subjected to any detriment by any act, or any deliberate failure to act, by his employer done on the ground that the worker has made a protected disclosure.”
Analysis:
The disclosure identifies that NHS staff may raise public-interest concerns about AI safety, unlawful data processing, patient confidentiality, unsafe triage, ambient voice errors, inadequate training, digital exclusion, or misleading productivity claims.
The concern is that AI-generated or AI-logged material may later be used to monitor, reframe, discipline, isolate, or discredit the worker after disclosure.
The disclosure identifies the protected-disclosure risk chain:
worker raises AI concern → employer reviews AI logs / usage / outputs / prompts → AI-derived material used against worker → detriment follows.
The Section 47B concern is that staff must be protected where they raise AI, patient safety, confidentiality, equality, or governance concerns.
The disclosure therefore identifies the need for AI evidence protocols, protected-disclosure safeguards, and restrictions on retaliatory use of AI-derived records.
IX.3 Employment Rights Act 1996, Section 98 — Fairness in Dismissal
Source:
Employment Rights Act 1996, Section 98 — General fairness in dismissal.
Material source: legislation.gov.uk — Employment Rights Act 1996, Section 98.
URL: https://www.legislation.gov.uk/ukpga/1996/18/section/98
Verbatim / principle:
An employer must show the reason for dismissal and that it falls within a potentially fair reason; fairness is assessed having regard to the reason shown and whether the employer acted reasonably in all the circumstances.
Analysis:
The disclosure identifies that NHS AI systems may create staff-facing records capable of later disciplinary or dismissal reliance.
Those records may include AI-use logs, prompts, generated outputs, access histories, audit trails, telemetry, productivity analytics, verification records, override histories, and AI-derived investigation material.
The Section 98 concern is that dismissal cannot be fair where the worker is judged on AI-derived material that they cannot inspect, understand, challenge, or contextualise.
The disclosure further identifies that fairness requires evidence of training, policy, role clarity, system accuracy, audit interpretation, human review, and whether the alleged error was human, AI-generated, system-generated, or caused by unclear deployment architecture.
The disclosure therefore identifies AI-derived disciplinary evidence as requiring traceability, disclosure, and human fairness safeguards before employment consequences are imposed.
IX.4 Employment Rights Act 1996, Section 103A — Protected Disclosure Dismissal
Source:
Employment Rights Act 1996, Section 103A — Protected disclosure dismissal.
Material source: legislation.gov.uk — Employment Rights Act 1996, Section 103A.
URL: https://www.legislation.gov.uk/ukpga/1996/18/section/103A
Verbatim / principle:
An employee who is dismissed shall be regarded as unfairly dismissed if the reason, or principal reason, for the dismissal is that the employee made a protected disclosure.
Analysis:
The disclosure identifies that NHS AI deployment creates whistleblowing risk because staff may reasonably disclose concerns about unsafe AI systems, patient-data exposure, poor training, AI hallucination, under-triage, ambient voice inaccuracies, unlawful processing, or staff liability displacement.
The Section 103A concern is engaged where a worker is dismissed after raising such concerns and the employer relies on AI-derived logs, outputs, audit trails, productivity records, or performance records to justify dismissal.
The disclosure asserts that where AI-derived material is used in dismissal contexts, the employer must disclose the full AI evidence chain.
That includes source material, prompt, output, system version, audit logic, human review, training record, policy in force, and whether the AI record is accurate.
The disclosure therefore identifies AI-derived dismissal evidence as a protected-disclosure risk area.
IX.5 Public Interest Disclosure Act 1998 — Whistleblowing Protection Framework
Source:
Public Interest Disclosure Act 1998.
Material source: legislation.gov.uk — Public Interest Disclosure Act 1998.
URL: https://www.legislation.gov.uk/ukpga/1998/23/contents
Verbatim / principle:
The Public Interest Disclosure Act 1998 amended the Employment Rights Act 1996 to provide protection for workers making qualifying disclosures in the public interest.
Analysis:
The disclosure identifies NHS AI deployment as capable of generating public-interest disclosure subject matter where systems may create patient safety risk, data protection breach, confidentiality degradation, equality failure, staff health and safety risk, misleading public claims, unlawful processing, lack of clinical safety assurance, or concealment of AI risks.
The disclosure further identifies that workers must be able to raise these issues without exposure to AI-mediated retaliation, audit misuse, disciplinary reframing, or evidential manipulation.
The PIDA concern is that NHS AI systems must include protected-disclosure routes that allow staff to report unsafe AI without fear that prompts, logs, telemetry, AI-generated records, or access histories will be weaponised against them.
The disclosure therefore identifies whistleblowing protection as essential to safe NHS AI governance.
IX.6 Health and Safety at Work etc. Act 1974, Section 2 — Employer Duty to Employees
Source:
Health and Safety at Work etc. Act 1974, Section 2 — General duties of employers to employees.
Material source: legislation.gov.uk — Health and Safety at Work etc. Act 1974, Section 2.
URL: https://www.legislation.gov.uk/ukpga/1974/37/section/2
Verbatim / principle:
“It shall be the duty of every employer to ensure, so far as is reasonably practicable, the health, safety and welfare at work of all his employees.”
Analysis:
The disclosure identifies that NHS AI deployment may create health, safety, and welfare risks for staff through workload pressure, unclear role boundaries, verification burden, AI hallucination risk, audit exposure, public criminal-threat messaging, inadequate training, and disciplinary uncertainty.
The concern applies where staff are expected to use, check, correct, approve, or rely on AI outputs without sufficient training, time, policy, support, or protection from unfair liability.
The Section 2 concern is that AI deployment must be assessed as a workplace-system change, not merely a productivity tool.
The disclosure therefore identifies that NHS employers must assess AI-related stress, workload, role ambiguity, competence, support, disciplinary boundaries, reasonable adjustments, and protected-disclosure protection before exposing staff to AI-mediated liability.
IX.7 Management of Health and Safety at Work Regulations 1999 — Risk Assessment
Source:
Management of Health and Safety at Work Regulations 1999, Regulation 3 — Risk assessment.
Material source: legislation.gov.uk — Management of Health and Safety at Work Regulations 1999, Regulation 3.
URL: https://www.legislation.gov.uk/uksi/1999/3242/regulation/3
Verbatim / principle:
Every employer shall make a suitable and sufficient assessment of the risks to the health and safety of employees and others arising out of work.
Analysis:
The disclosure identifies that NHS AI deployment changes work activities.
Staff may be required or encouraged to use AI systems that generate outputs, summaries, audit trails, prompts, classifications, patient-adjacent documents, and verification obligations.
The concern is that risk assessment must address AI verification burden, hallucination checking, clinical-output review, audit-log exposure, disciplinary uncertainty, training gaps, role ambiguity, stress, equality impact, workload changes, and staff confidence in rejecting unsafe AI output.
The disclosure therefore identifies that NHS AI implementation requires health-and-safety risk assessment for workers as well as clinical safety assessment for patients.
IX.8 HSE Management Standards — Work-Related Stress
Source:
Health and Safety Executive — Management Standards for work-related stress.
Material source: HSE — What are the Management Standards?
URL: https://www.hse.gov.uk/stress/standards/
Verbatim / principle:
The HSE Management Standards cover six key areas of work design: demands, control, support, relationships, role, and change.
Analysis:
The disclosure identifies that NHS AI deployment engages all six stress domains.
AI may increase demands if productivity claims lead to higher workloads. It may reduce control if tools are imposed. It may weaken support if training is inadequate. It may affect relationships where errors are disputed as human or machine-originated. It may create role ambiguity where staff become users, verifiers, editors, auditors, and liability endpoints. It may intensify change pressure through rapid rollout.
The disclosure further identifies that public warning language concerning dismissal or prison for inappropriate access intensifies stress where staff are simultaneously being placed into AI-mediated patient-data systems.
The HSE concern is therefore that NHS AI deployment must include visible stress and workload assessment, not merely user training.
IX.9 ACAS Code of Practice — Disciplinary and Grievance Procedures
Source:
ACAS Code of Practice on Disciplinary and Grievance Procedures.
Material source: ACAS — Code of Practice on disciplinary and grievance procedures.
URL: https://www.acas.org.uk/acas-code-of-practice-on-disciplinary-and-grievance-procedures
Verbatim / principle:
Employers should deal with disciplinary and grievance issues fairly, consistently, and without unreasonable delay.
Analysis:
The disclosure identifies that AI-derived material may be used in disciplinary or grievance contexts.
Such material may include prompts, outputs, access logs, AI-use records, telemetry, generated summaries, audit trails, and system interpretations.
The ACAS concern is that fair process requires the worker to understand the case, see the evidence, challenge the evidence, and explain context.
The disclosure asserts that where AI-derived records are relied upon, fairness requires disclosure of the raw record, AI-generated record, source data, system version, prompt, audit interpretation, human review, training record, and policy in force at the time.
The disclosure therefore identifies that AI evidence cannot be used in disciplinary procedures as if it were ordinary human-authored evidence.
IX.10 Common Law Implied Duty of Mutual Trust and Confidence
Source:
Common law employment duty of mutual trust and confidence.
Material source: Malik v Bank of Credit and Commerce International SA [1997] UKHL 23.
URL: https://www.bailii.org/uk/cases/UKHL/1997/23.html
Verbatim / principle:
An employer must not, without reasonable and proper cause, conduct itself in a manner likely to destroy or seriously damage the relationship of trust and confidence.
Analysis:
The disclosure identifies that NHS AI deployment may affect the employment relationship where staff are placed into AI-mediated systems without clear training, role boundaries, audit-log explanation, verification time, disciplinary safeguards, or protection from upstream system error.
The concern is intensified where public messaging warns staff of dismissal or prison for improper patient-record access while AI tools expand the volume and complexity of patient-adjacent processing.
The disclosure asserts that trust and confidence may be undermined where staff are expected to use AI outputs, check AI-generated material, accept AI-generated workflow records, and carry liability for systems they did not design, procure, configure, or govern.
The legal concern is that AI cannot be introduced as a productivity tool while the worker silently becomes the accountability endpoint for prompts, outputs, audit trails, telemetry, hallucinations, transcription errors, access logs, or system-generated records.
IX.11 Employer Common Law Duty of Care
Source:
Common law employer duty of care.
Material source: Walker v Northumberland County Council [1995] 1 All ER 737; general employer negligence principles.
URL: https://www.bailii.org/
Verbatim / principle:
An employer owes a duty to take reasonable care for the safety of employees, including protection from reasonably foreseeable harm.
Analysis:
The disclosure identifies foreseeable worker harm arising from AI deployment where staff are exposed to increased verification burden, unclear policy, audit surveillance, patient-data anxiety, disciplinary uncertainty, and public criminal-threat messaging.
The concern applies where AI tools produce outputs that staff must verify under pressure, including clinical summaries, ambient voice transcripts, generated correspondence, triage outputs, patient-adjacent notes, and administrative records.
The disclosure further identifies that foreseeable harm may include stress, anxiety, capability pressure, reputational damage, disciplinary exposure, and protected-disclosure detriment.
The duty of care concern is therefore that NHS employers must assess AI-related work risk before deployment, including training, workload, role clarity, support, error escalation, reasonable adjustments, and protection where the AI system creates or contributes to error.
X. Public Law, Procurement, Accountability, Continuity, and Sovereignty Layer
X.1 Public Law Rationality — Reasoned Decision-Making
Source:
Public law rationality / reasonableness principles.
Material source: Council of Civil Service Unions v Minister for the Civil Service [1985] AC 374; Associated Provincial Picture Houses Ltd v Wednesbury Corporation [1948] 1 KB 223.
URL: https://www.bailii.org/uk/cases/UKHL/1984/9.html
URL: https://www.bailii.org/ew/cases/EWCA/Civ/1947/1.html
Verbatim / principle:
Public authorities must act rationally, take relevant considerations into account, and avoid decisions so unreasonable that no reasonable public authority could have made them.
Analysis:
The disclosure identifies NHS AI deployment as a public-authority decision requiring rational assessment of relevant risks.
The relevant considerations include patient confidentiality, special-category health data, clinical safety, AI hallucination, triage error, ambient voice accuracy, accent validation, disability access, equality impact, staff training, audit exposure, processor chains, cloud dependency, telemetry, support access, cross-border risk, public trust, and sovereign exit capability.
The disclosure asserts that AI deployment cannot be rationally justified by productivity claims alone.
The relevant public-law question is whether NHS bodies considered the full consequence of inserting AI systems into patient access, clinical records, staff workflow, confidential medical processing, and later evidential reliance.
The disclosure therefore identifies rationality as engaged where public bodies deploy AI systems without showing the risk assessment, evidence base, safeguards, alternatives, and accountability map.
X.2 Public Law Proportionality — Intrusion Must Match Necessity
Source:
Public law proportionality principles, including rights-compatible public decision-making.
Material source: Human Rights Act 1998; Bank Mellat v HM Treasury (No 2) [2013] UKSC 39.
URL: https://www.legislation.gov.uk/ukpga/1998/42/contents
URL: https://www.bailii.org/uk/cases/UKSC/2013/39.html
Verbatim / principle:
A public measure affecting rights must pursue a legitimate aim and must not go further than necessary to achieve that aim.
Analysis:
The disclosure identifies proportionality as engaged where NHS AI processing interferes with privacy, confidentiality, dignity, equality, staff rights, and patient access.
The legitimate aim may be service improvement, administrative efficiency, clinical access, workforce support, or waiting-list reduction.
The proportionality question is whether the chosen AI method goes further than necessary.
The concern applies where patient data is processed through external AI systems, voice is captured, AI summaries enter records, telemetry is generated, support access exists, vendor chains expand, staff are audited, and patients are routed through AI systems without equivalent non-AI access.
The disclosure therefore identifies that proportionality requires a less-intrusive alternative analysis, including human routes, non-AI digital routes, local processing, minimised logging, restricted telemetry, stronger safeguards, and sovereign alternatives.
X.3 Public Law Procedural Fairness — Fair Process Before Rights Are Affected
Source:
Public law procedural fairness / natural justice.
Material source: R v Secretary of State for the Home Department, ex parte Doody [1993] UKHL 8.
URL: https://www.bailii.org/uk/cases/UKHL/1993/8.html
Verbatim / principle:
Where an administrative decision affects rights, interests, or legitimate expectations, fairness may require that the affected person is given sufficient information and a meaningful opportunity to respond.
Analysis:
The disclosure identifies procedural fairness as engaged where AI systems affect patient access, clinical records, complaint outcomes, staff disciplinary material, audit exposure, employment position, or evidential reliance.
The concern is that patients and workers may be affected by AI-generated or AI-mediated outputs without knowing that AI was involved, what it produced, what source data was used, who reviewed it, whether it was corrected, or how to challenge it.
The disclosure asserts that fairness requires visibility of the AI chain where AI material affects rights or interests.
The disclosure therefore identifies that NHS AI deployment must include notice, explanation, access, correction, objection, human review, preservation, and challenge routes before AI-derived material is relied upon.
X.4 Legitimate Expectation — Public Trust in Medical Confidentiality and Human Access
Source:
Public law legitimate expectation.
Material source: R v North and East Devon Health Authority, ex parte Coughlan [1999] EWCA Civ 1871.
URL: https://www.bailii.org/ew/cases/EWCA/Civ/1999/1871.html
Verbatim / principle:
A legitimate expectation may arise where a public authority’s representation, practice, or established relationship gives rise to an expectation that it will act in a particular way.
Analysis:
The disclosure identifies that NHS patients hold a legitimate expectation that confidential medical information is used for care within trusted healthcare governance, not silently transformed into AI prompts, transcripts, summaries, telemetry, support records, model-monitoring signals, or externally administered processing layers without clear notice.
The disclosure further identifies an expectation that access to NHS care will remain clinically safe, humanly reviewable, accessible, and not dependent on opaque AI systems.
The legitimate-expectation concern is that NHS AI deployment alters the practical relationship between patient, clinician, record, worker, infrastructure, and vendor without sufficient public explanation.
The disclosure therefore identifies that patients should not discover after deployment that AI systems have become embedded into access, documentation, triage, record formation, or confidential processing pathways.
X.5 Public Law Duty to Give Reasons — Explain the AI Decision Architecture
Source:
Public law duty to give reasons where fairness, statutory context, or impact requires explanation.
Material source: R v Secretary of State for the Home Department, ex parte Doody [1993] UKHL 8.
URL: https://www.bailii.org/uk/cases/UKHL/1993/8.html
Verbatim / principle:
Fairness may require reasons to be given where a decision substantially affects a person’s rights or interests.
Analysis:
The disclosure identifies that AI-mediated decisions and outputs require explanation where they affect patient routing, clinical records, access to care, complaints, staff audit exposure, disciplinary action, protected disclosure, or legal evidence.
The concern is not limited to a final decision letter.
The reasons may sit inside the AI pathway: symptom inputs, triage logic, prompts, generated output, system settings, model version, human review, override rules, escalation thresholds, and audit interpretation.
The disclosure therefore identifies that public bodies must be able to explain how AI systems acted, what information was used, what output was generated, who reviewed it, and how the final consequence was reached.
Without that explanation, AI becomes a hidden reasons layer.
X.6 Public-Sector Transparency — Algorithmic Transparency Recording Standard
Source:
Algorithmic Transparency Recording Standard.
Material source: GOV.UK — Algorithmic Transparency Recording Standard hub.
URL: https://www.gov.uk/government/collections/algorithmic-transparency-recording-standard-hub
Verbatim / principle:
The Algorithmic Transparency Recording Standard is a framework for public-sector organisations to provide information about algorithmic tools used to support decisions.
Analysis:
The disclosure identifies NHS AI deployment as requiring public transparency where algorithmic or AI systems support patient access, triage, clinical documentation, staff workflow, audit, prioritisation, or operational decision-making.
The relevant information includes system name, supplier, purpose, decision supported, human oversight, data used, data protection assessment, equality assessment, risks, mitigations, appeals, and contact route.
The disclosure asserts that public-sector algorithmic transparency must apply before dependency forms, not only after controversy.
The concern is that patients and workers cannot understand, challenge, or trust AI systems if the public record does not show what tools are in use and what they affect.
X.7 Procurement Act 2023 — Public Procurement Accountability
Source:
Procurement Act 2023.
Material source: legislation.gov.uk — Procurement Act 2023.
URL: https://www.legislation.gov.uk/ukpga/2023/54/contents
Verbatim / principle:
The Procurement Act 2023 establishes a statutory framework for public procurement, including transparency, value for money, integrity, public benefit, and accountability.
Analysis:
The disclosure identifies NHS AI procurement as requiring scrutiny beyond headline price, pilot performance, vendor claims, or deployment scale.
The relevant procurement risks include vendor dependency, cloud lock-in, processor chains, exit cost, data portability, audit access, clinical safety evidence, DPIA evidence, equality assessment, cybersecurity assurance, medical-device classification, model-monitoring obligations, training burden, and long-term operational cost.
The disclosure asserts that value for money cannot be assessed where the public is shown projected time savings but not the evidence base, hidden verification cost, rework burden, staff training cost, clinical safety risk, data-governance risk, or exit-risk cost.
The procurement concern is that AI contracts may create dependency before Parliament, patients, staff, and the public can assess the full public-interest cost.
X.8 Managing Public Money — Regularity, Propriety, Value for Money, and Feasibility
Source:
HM Treasury — Managing Public Money.
Material source: GOV.UK — Managing Public Money.
URL: https://www.gov.uk/government/publications/managing-public-money
Verbatim / principle:
Public funds should be used with regularity, propriety, value for money, and feasibility.
Analysis:
The disclosure identifies that NHS AI spending must be assessed against actual public value, not speculative productivity claims.
The concern applies where claimed benefits rely on self-reported time saving, narrow pilots, early-adopter behaviour, non-comparable baselines, unmeasured verification burden, or unpriced downstream risk.
The disclosure asserts that AI value claims must include full cost: licensing, integration, training, clinical safety assurance, DPIAs, equality assessments, cybersecurity, support, audit, correction, incident handling, rework, staff stress, procurement lock-in, and exit.
The Managing Public Money concern is that public funds cannot be justified by efficiency claims that omit governance cost and risk transfer.
X.9 Cabinet Office Technology Code of Practice — Open Standards, Reuse, Security, and Exit
Source:
Cabinet Office / Central Digital and Data Office — Technology Code of Practice.
Material source: GOV.UK — Technology Code of Practice.
URL: https://www.gov.uk/guidance/the-technology-code-of-practice
Verbatim / principle:
The Technology Code of Practice sets expectations for public-sector technology, including user needs, open standards, security, interoperability, and avoiding unnecessary lock-in.
Analysis:
The disclosure identifies that NHS AI deployment must be assessed against public-sector technology principles.
The relevant concerns include whether systems meet patient and staff needs, whether they are accessible, interoperable, secure, auditable, open enough to permit switching, and free from avoidable lock-in.
The disclosure asserts that AI systems create heightened lock-in because they may become embedded into workflow, records, training, procurement, audit, and operational dependency.
The concern is that once AI infrastructure becomes normalised, exit becomes clinically, financially, operationally, and politically difficult.
The disclosure therefore identifies sovereign exit, portability, interoperability, and open standards as public-sector technology duties, not optional technical preferences.
X.10 Cabinet Office Sourcing Playbook — Outsourcing, Risk Allocation, and Supplier Dependency
Source:
Cabinet Office — Sourcing Playbook.
Material source: GOV.UK — The Sourcing Playbook.
URL: https://www.gov.uk/government/publications/the-sourcing-playbook
Verbatim / principle:
Public-sector outsourcing requires careful commercial strategy, risk allocation, delivery model assessment, contract management, and supplier-risk management.
Analysis:
The disclosure identifies NHS AI deployment as an outsourcing and supplier-dependency risk where core healthcare functions become dependent on external AI, SaaS, cloud, analytics, telemetry, and support infrastructure.
The relevant risks include loss of internal capability, supplier lock-in, price escalation, data-portability barriers, degraded bargaining position, limited audit access, foreign legal exposure, service continuity risk, and inability to exit without disruption.
The disclosure asserts that AI dependency is not merely a procurement issue.
It becomes a public-health continuity issue where patient access, records, triage, staff workflow, and operational scheduling depend on externally controlled systems.
The disclosure therefore identifies supplier dependency and risk allocation as central to NHS AI accountability.
X.11 National Cyber Security Centre Cloud Security Principles — Cloud and SaaS Assurance
Source:
National Cyber Security Centre — Cloud Security Principles.
Material source: NCSC — Cloud security guidance.
URL: https://www.ncsc.gov.uk/collection/cloud
Verbatim / principle:
Cloud services should be assessed against security principles including data protection in transit and at rest, asset protection, separation, governance, operational security, personnel security, secure development, supply-chain security, identity and authentication, external interfaces, secure service administration, audit, and customer control.
Analysis:
The disclosure identifies that NHS AI deployment may rely on cloud, SaaS, AI model, speech-to-text, telemetry, analytics, support, and monitoring services.
The cybersecurity concern is not limited to hacking.
It includes authorised access, administrator access, support access, API access, telemetry extraction, model-monitoring records, logs, cloud jurisdiction, operational control, audit capability, and customer ability to enforce deletion, restriction, access control, and exit.
The disclosure asserts that NHS AI cybersecurity must assess the whole service chain, including system exhaust.
The disclosure therefore identifies cloud assurance as essential where confidential medical data or AI-derived health information is processed outside direct NHS-controlled infrastructure.
X.12 Business Continuity and Operational Resilience — Critical Healthcare Infrastructure
Source:
Business continuity and operational resilience principles for public services and critical healthcare systems.
Material source: Cabinet Office resilience guidance; NHS England emergency preparedness, resilience and response materials.
URL: https://www.gov.uk/government/collections/emergency-preparedness-resilience-and-response
URL: https://www.england.nhs.uk/ourwork/eprr/
Verbatim / principle:
Public services should plan for continuity, resilience, disruption, recovery, and critical service protection.
Analysis:
The disclosure identifies NHS AI systems as potential critical dependencies where they become embedded into access, triage, documentation, scheduling, staff workflow, and records.
The concern is that AI failure, supplier withdrawal, licence suspension, price shock, cyber incident, cloud outage, model degradation, export restriction, contract dispute, or vendor policy change may disrupt NHS service delivery.
The disclosure asserts that AI deployment must include fallback routes, manual continuity, non-AI access, data-portability, exit planning, service-recovery testing, and resilience assurance.
The disclosure therefore identifies public-sector AI dependency as a continuity risk, not merely an innovation risk.
X.13 Sovereign Control and Exit Risk — Foreign-Controlled Infrastructure Dependency
Source:
Public-sector sovereignty, resilience, supplier-dependency, and critical infrastructure governance principles.
Material source: UK government digital, procurement, cyber, and resilience frameworks.
URL: https://www.gov.uk/government/collections/algorithmic-transparency-recording-standard-hub
URL: https://www.gov.uk/guidance/the-technology-code-of-practice
URL: https://www.ncsc.gov.uk/collection/cloud
URL: https://www.gov.uk/government/publications/the-sourcing-playbook
Verbatim / principle:
Public-sector technology should remain accountable, secure, resilient, auditable, interoperable, and capable of responsible management across its lifecycle.
Analysis:
The disclosure identifies sovereign control as engaged where NHS AI systems rely on foreign-controlled cloud, SaaS, AI model, telemetry, support, identity, analytics, or infrastructure providers.
The issue is not anti-technology.
The issue is whether the NHS retains control over patient data, execution logic, records, audit trails, service continuity, pricing exposure, exit route, supplier substitution, and legal accountability.
The disclosure asserts that a healthcare system cannot become dependent on infrastructure that can be repriced, degraded, withdrawn, contractually constrained, remotely administered, legally compelled, or politically leveraged outside direct NHS control.
The disclosure therefore identifies sovereign exit risk as a public-interest issue where AI systems process confidential medical data and become embedded into national healthcare operations.
XI. Evidential, Procedural Fairness, Disclosure, Preservation, and AI-Reliability Layer
XI.1 Natural Justice — Right to Know and Answer the Case
Source:
Common law natural justice and procedural fairness.
Material source: R v Secretary of State for the Home Department, ex parte Doody [1993] UKHL 8.
URL: https://www.bailii.org/uk/cases/UKHL/1993/8.html
Verbatim / principle:
Fairness requires that a person affected by a decision is given sufficient information to understand the case and a meaningful opportunity to respond.
Analysis:
The disclosure identifies natural justice as engaged wherever AI-generated or AI-mediated material is relied upon against a patient, worker, complainant, litigant, clinician, whistleblower, or data subject.
The relevant material may include AI triage outputs, ambient voice transcripts, AI-generated clinical summaries, prompts, staff usage logs, audit trails, access histories, telemetry, AI-assisted investigation notes, complaint-handling records, disciplinary material, and tribunal evidence.
The disclosure asserts that a person cannot fairly answer a case if the evidence against them is AI-derived but the underlying source, prompt, system version, model logic, human review, edit history, audit interpretation, and processing chain are withheld.
The procedural concern is therefore that AI-derived material must be disclosed in a form capable of being understood, challenged, corrected, and tested.
XI.2 Evidential Reliability — Source-to-Output Traceability
Source:
Evidential reliability and procedural fairness principles.
Material source: common law evidential fairness; tribunal and court procedural fairness principles.
URL: https://www.judiciary.uk/courts-and-tribunals/employment-tribunal/
URL: https://www.justice.gov.uk/courts/procedure-rules/civil
Verbatim / principle:
Evidence relied upon in legal, disciplinary, regulatory, complaint, or decision-making processes must be capable of being tested for reliability, relevance, authenticity, and weight.
Analysis:
The disclosure identifies source-to-output traceability as a core AI evidence requirement.
The issue is that AI systems may produce summaries, classifications, transcripts, decisions, recommendations, and audit records without preserving the full path from original input to final output.
The relevant chain includes:
source material → prompt / input → AI system → model or rules layer → output → human review → edit history → final record → later reliance.
The disclosure asserts that AI-derived evidence is procedurally unsafe where the affected person cannot see what the AI received, what it generated, what was changed, who approved it, what version was used, and how the final record was produced.
The disclosure therefore identifies source-to-output traceability as essential before AI material is relied upon in healthcare, employment, complaint, disciplinary, tribunal, regulatory, or legal contexts.
XI.3 Disclosure Duties — AI-Derived Material Must Be Disclosed Where Relevant
Source:
Disclosure principles in civil, tribunal, complaint, and regulatory procedures.
Material source: Civil Procedure Rules Part 31; Employment Tribunals Rules of Procedure; public-law fairness principles.
URL: https://www.justice.gov.uk/courts/procedure-rules/civil/rules/part31
URL: https://www.gov.uk/government/publications/employment-tribunal-procedure-rules
Verbatim / principle:
Relevant documents and material capable of supporting or undermining a party’s case may be disclosable, subject to the applicable procedural rules.
Analysis:
The disclosure identifies that AI-derived records may become disclosable where they are relevant to patient harm, staff discipline, protected disclosure, clinical complaint, data rights, tribunal proceedings, negligence, equality claim, public-law challenge, or regulatory investigation.
Relevant AI-derived material may include prompts, outputs, transcripts, logs, metadata, audit trails, model versions, system settings, support tickets, telemetry, correction histories, human-review notes, and source documents used by AI tools.
The disclosure asserts that institutions cannot rely on an AI-generated final record while withholding the underlying AI process that produced it.
The disclosure concern is that AI systems create hidden evidence layers that may support, undermine, explain, or contradict the visible record.
Therefore, disclosure duties must apply to the AI chain where AI-derived material affects rights, obligations, records, liability, disciplinary action, or legal proof.
XI.4 Preservation Duties — AI Records Must Not Be Lost, Overwritten, or Normalised
Source:
Procedural preservation duties and data-protection preservation principles.
Material source: Data Protection Act 2018, Section 173; civil and tribunal disclosure principles.
URL: https://www.legislation.gov.uk/ukpga/2018/12/section/173
URL: https://www.justice.gov.uk/courts/procedure-rules/civil/rules/part31
Verbatim / principle:
Information must not be altered, erased, destroyed, concealed, or made unavailable where a person would be entitled to receive it or where it is relevant to proceedings or rights.
Analysis:
The disclosure identifies preservation as a core AI governance requirement because AI systems may overwrite, regenerate, summarise, normalise, purge, or collapse records into final outputs.
The risk applies to ambient voice audio status, transcripts, draft summaries, final summaries, triage inputs, triage outputs, prompts, generated text, staff edits, audit logs, telemetry, support records, model-monitoring records, system versions, and correction histories.
The disclosure asserts that once a complaint, dispute, subject access request, protected disclosure, disciplinary issue, patient-safety concern, tribunal claim, legal claim, or regulatory question arises, relevant AI-derived material must be preserved.
The procedural concern is that AI systems may erase the evidence chain by design unless retention and litigation-hold rules are imposed.
The disclosure therefore identifies preservation controls as required before AI-derived material can safely enter healthcare or employment systems.
XI.5 Authenticity and Metadata — AI Evidence Requires Provenance
Source:
Evidential authenticity and provenance principles.
Material source: common law evidence principles; procedural disclosure practice; digital evidence handling principles.
URL: https://www.justice.gov.uk/courts/procedure-rules/civil
Verbatim / principle:
Digital evidence requires provenance sufficient to establish origin, integrity, timing, authorship, alteration, and reliability.
Analysis:
The disclosure identifies that AI-generated material may appear authoritative while lacking visible authorship and provenance.
The relevant provenance questions include:
Who created the record?
Was it generated by AI, edited by a clinician, imported by staff, or produced by a vendor system?
What source material was used?
What prompt or input generated it?
What system version was active?
Was the output reviewed?
Was it changed?
Was the raw material retained?
Was the final record corrected?
Was metadata preserved?
The disclosure asserts that AI evidence without provenance is vulnerable to misattribution.
The procedural concern is that AI may produce records that look human-authored, clinically approved, or institutionally verified when they are actually system-generated, partially edited, or unsupported by preserved source material.
The disclosure therefore identifies metadata and provenance as essential AI evidence safeguards.
XI.6 Human Review — Meaningful Review Cannot Be Assumed
Source:
Procedural fairness, data-protection, and clinical safety principles requiring meaningful human oversight where automated systems affect rights or safety.
Material source: UK GDPR Article 22; clinical safety governance; public-law fairness principles.
URL: https://www.legislation.gov.uk/eur/2016/679/article/22
URL: https://www.england.nhs.uk/long-read/digital-clinical-safety-assurance/
Verbatim / principle:
Where automated or AI-mediated outputs affect people, human review must be meaningful, informed, and capable of altering the outcome.
Analysis:
The disclosure identifies that AI systems are often described as support tools, but the practical safeguard depends on whether human review is real.
The concern is that clinicians, administrators, investigators, managers, or HR staff may accept AI outputs because of time pressure, workload, interface design, automation bias, insufficient training, or lack of access to source material.
The disclosure asserts that human review is not meaningful where the reviewer cannot see the original input, transcript, prompt, system confidence, model limitation, source document, edit history, or known error risks.
The disclosure therefore identifies that NHS AI governance must define who reviews AI outputs, what they review, how much time they have, what authority they have to reject the output, and how disagreement is recorded.
XI.7 Automation Bias — AI Outputs May Be Over-Relied Upon
Source:
Clinical safety, human factors, and AI governance principles concerning automation bias and overreliance.
Material source: NHS clinical safety assurance; NICE evidence standards; MHRA software and AI guidance.
URL: https://www.england.nhs.uk/long-read/digital-clinical-safety-assurance/
URL: https://www.nice.org.uk/corporate/ecd7
URL: https://www.gov.uk/government/publications/software-and-artificial-intelligence-ai-as-a-medical-device/software-and-artificial-intelligence-ai-as-a-medical-device
Verbatim / principle:
Digital health technologies must be assessed for risk, evidence, human factors, safety, and appropriate use.
Analysis:
The disclosure identifies automation bias as a foreseeable risk in NHS AI deployment.
Staff may defer to AI triage, AI summaries, AI transcripts, AI-generated letters, audit flags, risk classifications, or productivity outputs because the system appears authoritative, integrated, official, or time-saving.
The risk is intensified where workload pressure, staffing shortages, national rollout pressure, and productivity claims encourage reliance on AI output.
The disclosure asserts that automation bias may convert a nominally advisory tool into a practical decision-maker.
The procedural concern is that where AI outputs are later relied upon, the institution must show how overreliance was prevented, how staff were trained to challenge outputs, and how errors were detected and corrected.
XI.8 Litigation Prejudice — AI Systems May Create Hidden Material Relevant to Proceedings
Source:
Civil, tribunal, and public-law procedural fairness principles.
Material source: Civil Procedure Rules; Employment Tribunal procedure; common law fairness.
URL: https://www.justice.gov.uk/courts/procedure-rules/civil
URL: https://www.gov.uk/government/publications/employment-tribunal-procedure-rules
Verbatim / principle:
A party must have a fair opportunity to know, obtain, test, and answer relevant material affecting proceedings.
Analysis:
The disclosure identifies litigation prejudice where AI-derived material exists but is not disclosed, preserved, identified, or understood as evidence.
This may apply where AI tools are used to generate records, summarise events, draft letters, triage complaints, prepare HR documents, analyse evidence, produce timelines, review patient records, or support legal decision-making.
The concern is that one party may rely on AI-generated material while the other party only sees the polished final document.
The disclosure asserts that AI-assisted documents may conceal source selection, omitted context, hallucinated content, summarisation choices, prompt framing, and system-generated assumptions.
The procedural concern is therefore that AI-assisted material used in legal or quasi-legal processes must be identified, preserved, and disclosed where it affects the fairness of proceedings.
XI.9 Complaint Fairness — AI Involvement Must Be Visible in NHS Complaints
Source:
NHS complaint-handling fairness principles and public-law accountability.
Material source: NHS complaints procedure; Parliamentary and Health Service Ombudsman principles.
URL: https://www.nhs.uk/nhs-services/how-to-complain-to-the-nhs/
URL: https://www.ombudsman.org.uk/about-us/our-principles
Verbatim / principle:
Complaints should be investigated properly, fairly, transparently, and with an evidence-based explanation.
Analysis:
The disclosure identifies that NHS AI systems may become relevant to patient complaints where care access, triage, clinical notes, appointment routing, voice capture, record accuracy, or communication was AI-mediated.
The concern is that complaint responses may address only the visible human or administrative action while omitting AI involvement.
The disclosure asserts that a complaint cannot be properly investigated if AI triage output, ambient voice transcript, AI summary, model version, audit trail, correction history, or human-review note is not obtained.
The procedural concern is that NHS complaints must include an AI evidence review where AI systems formed part of the pathway being complained about.
XI.10 Tribunal Fairness — AI-Derived Employment Material Requires Disclosure and Challenge
Source:
Employment Tribunal Rules of Procedure and overriding objective.
Material source: GOV.UK — Employment Tribunal procedure rules.
URL: https://www.gov.uk/government/publications/employment-tribunal-procedure-rules
Verbatim / principle:
Employment Tribunal procedure requires cases to be dealt with fairly and justly.
Analysis:
The disclosure identifies tribunal fairness as engaged where AI-derived staff records are used in disciplinary, grievance, dismissal, protected-disclosure, discrimination, capability, conduct, or performance disputes.
Relevant AI-derived material may include staff prompts, Copilot usage, audit logs, access histories, generated notes, AI-assisted investigation documents, automated summaries, telemetry, training records, system warnings, and disciplinary evidence derived from AI systems.
The disclosure asserts that workers must be able to test whether the AI-derived record is accurate, complete, contextual, lawful, preserved, and fairly interpreted.
The procedural concern is that tribunal evidence may become unsafe where AI-derived material is presented as ordinary employer evidence without disclosing the AI system that generated, shaped, filtered, or interpreted it.
XI.11 Burden of Verification — AI Shifts Evidential Labour Onto Patients and Staff
Source:
Procedural fairness, clinical safety, data-subject rights, and employment fairness principles.
Material source: UK GDPR Articles 15–16; clinical safety governance; employment procedural fairness.
URL: https://www.legislation.gov.uk/eur/2016/679/article/15
URL: https://www.legislation.gov.uk/eur/2016/679/article/16
URL: https://www.acas.org.uk/acas-code-of-practice-on-disciplinary-and-grievance-procedures
Verbatim / principle:
Rights to access, correction, fair process, and safe care must be practical and effective, not merely theoretical.
Analysis:
The disclosure identifies that AI deployment may shift verification burden onto patients and staff.
Patients may have to detect inaccurate summaries, mistranscribed consultations, wrong triage outputs, omitted symptoms, incorrect routing, or AI-derived clinical-record errors.
Staff may have to verify AI summaries, check hallucinations, correct transcripts, review prompts, validate outputs, and defend themselves against AI-generated audit records.
The disclosure asserts that rights are weakened where the person affected must discover and correct AI error without being told AI was involved or given access to the full chain.
The procedural concern is that AI systems can silently externalise verification labour onto the people least able to see the system.
XI.12 Audit-Trail Fairness — Logs Are Not Neutral Evidence Unless Interpreted Correctly
Source:
Digital evidence, employment fairness, data-protection accountability, and clinical governance principles.
Material source: UK GDPR Article 5 accountability; ACAS fairness; clinical safety assurance.
URL: https://www.legislation.gov.uk/eur/2016/679/article/5
URL: https://www.acas.org.uk/acas-code-of-practice-on-disciplinary-and-grievance-procedures
URL: https://www.england.nhs.uk/long-read/digital-clinical-safety-assurance/
Verbatim / principle:
Records relied upon for accountability must be accurate, contextual, and capable of fair interpretation.
Analysis:
The disclosure identifies that audit logs, access histories, telemetry, prompt records, and AI-use records may appear objective but require interpretation.
A log may show access, but not purpose.
A prompt may show user input, but not system instruction.
An output may show generated text, but not correctness.
Telemetry may show usage, but not competence.
A correction may show editing, but not whether the AI was wrong.
The disclosure asserts that AI audit records must not be treated as self-explanatory proof of misconduct, competence, negligence, non-compliance, or intent.
The procedural concern is that audit-trail material must be interpreted with training records, policy context, system design, role expectation, workload, human review, and known AI limitations.
XII. International Human Rights, Privacy, Bioethics, and Business-Human-Rights Layer
XII.1 Universal Declaration of Human Rights, Article 12 — Privacy, Family, Home, and Correspondence
Source:
Universal Declaration of Human Rights, Article 12.
Material source: United Nations — Universal Declaration of Human Rights.
URL: https://www.un.org/en/about-us/universal-declaration-of-human-rights
Verbatim / principle:
“No one shall be subjected to arbitrary interference with his privacy, family, home or correspondence.”
Analysis:
The disclosure identifies NHS AI deployment as engaging international privacy principles where patient medical information, symptoms, consultation speech, digital access behaviour, clinical notes, AI-generated summaries, triage outputs, audit logs, telemetry, and staff-use records are processed through AI-mediated systems.
The concern is that privacy interference may become arbitrary where the patient or worker cannot see the processing pathway, vendor chain, execution location, retention rule, support-access route, model-monitoring function, objection route, or correction route.
The disclosure asserts that medical privacy is not limited to database storage.
In AI systems, privacy is affected by capture, transformation, inference, classification, logging, retention, support access, and later reliance.
The UDHR concern therefore supports the disclosure position that confidential medical and worker information must not be absorbed into opaque AI processing architecture without clear necessity, transparency, safeguard, and remedy.
XII.2 Universal Declaration of Human Rights, Article 19 — Freedom to Seek, Receive, and Impart Information
Source:
Universal Declaration of Human Rights, Article 19.
Material source: United Nations — Universal Declaration of Human Rights.
URL: https://www.un.org/en/about-us/universal-declaration-of-human-rights
Verbatim / principle:
“Everyone has the right to freedom of opinion and expression.”
“This right includes freedom to hold opinions without interference and to seek, receive and impart information and ideas through any media…”
Analysis:
The disclosure identifies Article 19 as engaged where patients, staff, clinicians, whistleblowers, researchers, journalists, litigants, and members of the public seek, receive, or impart information about NHS AI deployment.
The concern applies to public-interest speech about patient-data processing, AI safety, triage risk, ambient voice capture, staff exposure, equality impact, procurement dependency, sovereign control, vendor access, and misleading public claims.
The disclosure asserts that AI governance must not suppress, chill, discredit, or procedurally punish those who raise concerns about public healthcare AI systems.
The Article 19 concern therefore reinforces the public-interest character of disclosure concerning AI systems deployed into national healthcare infrastructure.
XII.3 International Covenant on Civil and Political Rights, Article 17 — Privacy Protection
Source:
International Covenant on Civil and Political Rights, Article 17.
Material source: OHCHR — International Covenant on Civil and Political Rights.
URL: https://www.ohchr.org/en/instruments-mechanisms/instruments/international-covenant-civil-and-political-rights
Verbatim / principle:
“No one shall be subjected to arbitrary or unlawful interference with his privacy, family, home or correspondence.”“Everyone has the right to the protection of the law against such interference or attacks.”
Analysis:
The disclosure identifies ICCPR Article 17 as engaged by AI processing of confidential medical information and worker records inside public healthcare systems.
The disclosure asserts that interference may be unlawful or arbitrary where processing is opaque, disproportionate, excessive, undisclosed, unsupported by adequate safeguards, or incapable of effective challenge.
The concern applies to AI triage, ambient voice systems, AI scribing, clinical summaries, patient-routing outputs, staff audit logs, Copilot-style records, telemetry, vendor support access, and model-monitoring data.
The ICCPR concern therefore reinforces that NHS AI systems must be capable of legal protection, challenge, access, correction, and accountability across the full processing chain.
XII.4 International Covenant on Economic, Social and Cultural Rights, Article 12 — Right to the Highest Attainable Standard of Health
Source:
International Covenant on Economic, Social and Cultural Rights, Article 12.
Material source: OHCHR — International Covenant on Economic, Social and Cultural Rights.
URL: https://www.ohchr.org/en/instruments-mechanisms/instruments/international-covenant-economic-social-and-cultural-rights
Verbatim / principle:
“The States Parties to the present Covenant recognize the right of everyone to the enjoyment of the highest attainable standard of physical and mental health.”
Analysis:
The disclosure identifies the right to health as engaged where AI systems affect access to care, triage routing, clinical documentation, appointment pathways, patient communication, disability access, and health-record accuracy.
The concern is that AI deployment may reduce healthcare quality where systems misroute patients, under-triage symptoms, mistranscribe consultations, omit red flags, exclude digitally disadvantaged groups, or create inaccurate records that influence future care.
The disclosure asserts that AI cannot be justified as healthcare improvement unless the deployment proves safety, accessibility, equality, clinical reliability, patient remedy, and human fallback.
The right-to-health concern therefore supports the disclosure position that AI deployment in healthcare must improve access and safety in practice, not merely promise administrative efficiency.
XII.5 International Covenant on Economic, Social and Cultural Rights, Article 7 — Just and Favourable Conditions of Work
Source:
International Covenant on Economic, Social and Cultural Rights, Article 7.
Material source: OHCHR — International Covenant on Economic, Social and Cultural Rights.
URL: https://www.ohchr.org/en/instruments-mechanisms/instruments/international-covenant-economic-social-and-cultural-rights
Verbatim / principle:
States recognise the right of everyone to the enjoyment of just and favourable conditions of work.
Analysis:
The disclosure identifies staff-facing AI deployment as engaging work-condition principles where workers are required to use, verify, correct, or rely on AI systems under pressure.
The concern applies to verification burden, hallucination checking, audit exposure, unclear liability, inadequate training, prompt discipline, performance analytics, workflow acceleration, public criminal-threat messaging, and AI-derived disciplinary records.
The disclosure asserts that AI systems must not transfer system risk onto workers while withholding system transparency, training, role clarity, workload assessment, and protected-disclosure safeguards.
The Article 7 concern therefore supports the position that healthcare AI must be governed as a workplace-system change, not only as a technical upgrade.
XII.6 Council of Europe Convention 108+ — Data Protection, Dignity, and Fundamental Freedoms
Source:
Council of Europe Convention 108+ — modernised Convention for the Protection of Individuals with Regard to the Processing of Personal Data.
Material source: Council of Europe — Convention 108+.
URL: https://www.coe.int/en/web/data-protection/convention108/modernised
Verbatim / principle:
Convention 108+ protects individuals with regard to the processing of personal data and supports respect for privacy, dignity, and fundamental freedoms.
Analysis:
The disclosure identifies Convention 108+ principles as engaged where NHS AI systems process personal data at scale, including special-category health data and worker data.
The concern applies to lawfulness, fairness, transparency, purpose limitation, minimisation, accuracy, storage limitation, security, accountability, and rights over automated or AI-mediated processing.
The disclosure asserts that healthcare AI creates intensified data-protection risk because data is not only stored but transformed into outputs, classifications, summaries, logs, telemetry, audit trails, and operational decisions.
Convention 108+ therefore reinforces the disclosure position that AI-era data protection must govern the acting data chain, not only the resting data store.
XII.7 OECD Privacy Guidelines — Collection Limitation, Purpose Specification, Use Limitation, Security, Openness, Participation, and Accountability
Source:
OECD Privacy Guidelines.
Material source: OECD — OECD Guidelines on the Protection of Privacy and Transborder Flows of Personal Data.
URL: https://www.oecd.org/sti/ieconomy/oecd_privacy_framework.pdf
Verbatim / principle:
The OECD privacy framework includes principles of collection limitation, data quality, purpose specification, use limitation, security safeguards, openness, individual participation, and accountability.
Analysis:
The disclosure identifies OECD privacy principles as directly engaged by NHS AI deployment.
The concern is that AI systems may collect more data than needed, generate new data from existing data, use data for secondary operational purposes, create hidden telemetry, expand support access, and make individual participation difficult.
The disclosure asserts that patients and workers must be able to know what data is collected, what purposes apply, what outputs are generated, who receives the data, how security is maintained, and how they can access or challenge records.
The OECD framework therefore supports the disclosure concern that AI systems must be open, accountable, limited, secure, and rights-accessible across the full lifecycle.
XII.8 UNESCO Universal Declaration on Bioethics and Human Rights, Article 5 — Autonomy and Individual Responsibility
Source:
UNESCO Universal Declaration on Bioethics and Human Rights, Article 5.
Material source: UNESCO — Universal Declaration on Bioethics and Human Rights.
URL: https://www.unesco.org/en/legal-affairs/universal-declaration-bioethics-and-human-rights
Verbatim / principle:
“The autonomy of persons to make decisions, while taking responsibility for those decisions and respecting the autonomy of others, is to be respected.”
Analysis:
The disclosure identifies patient autonomy as engaged where AI systems mediate healthcare access, symptom submission, triage, consultation capture, clinical summaries, and record formation.
The concern is that patient autonomy is weakened where AI processing occurs without clear notice, meaningful choice, accessible explanation, equivalent human route, objection route, or correction route.
The disclosure asserts that autonomy requires more than passive exposure to AI-enabled systems.
Patients must understand when AI is involved, what it does, what data it processes, whether outputs affect care, and how to refuse, correct, or request human review.
UNESCO Article 5 therefore supports the disclosure position that healthcare AI must preserve patient agency, not silently replace it with system-mediated processing.
XII.9 UNESCO Universal Declaration on Bioethics and Human Rights, Article 6 — Consent
Source:
UNESCO Universal Declaration on Bioethics and Human Rights, Article 6.
Material source: UNESCO — Universal Declaration on Bioethics and Human Rights.
URL: https://www.unesco.org/en/legal-affairs/universal-declaration-bioethics-and-human-rights
Verbatim / principle:
“Any preventive, diagnostic and therapeutic medical intervention is only to be carried out with the prior, free and informed consent of the person concerned.”
Analysis:
The disclosure identifies consent principles as engaged where AI systems process patient data in the context of diagnosis, triage, consultation, record formation, or clinical decision support.
The disclosure does not assert that every NHS processing activity requires consent as the legal basis under data protection law.
The disclosure identifies a separate medical-ethics concern: patients should be informed where AI materially participates in the capture, interpretation, summarisation, routing, or recording of their healthcare interaction.
The concern is that patients cannot give informed participation if AI involvement is hidden, generic, or explained only after processing occurs.
UNESCO Article 6 therefore supports the disclosure position that AI-mediated healthcare requires clear patient information, meaningful choice, and refusal routes where the AI function affects the medical interaction.
XII.10 UNESCO Universal Declaration on Bioethics and Human Rights, Article 9 — Privacy and Confidentiality
Source:
UNESCO Universal Declaration on Bioethics and Human Rights, Article 9.
Material source: UNESCO — Universal Declaration on Bioethics and Human Rights.
URL: https://www.unesco.org/en/legal-affairs/universal-declaration-bioethics-and-human-rights
Verbatim / principle:
“The privacy of the persons concerned and the confidentiality of their personal information should be respected.”
Analysis:
The disclosure identifies Article 9 as directly engaged by NHS AI systems processing confidential patient information.
The concern applies to symptoms, diagnosis, consultation speech, medication, disability information, safeguarding material, mental-health disclosure, triage answers, clinical notes, ambient voice transcripts, AI summaries, prompts, logs, telemetry, and support records.
The disclosure asserts that confidentiality must follow the data wherever it acts.
If confidential medical information is transformed into AI outputs, logs, summaries, transcripts, support tickets, telemetry, or model-monitoring records, those derived records must remain protected by confidentiality principles.
UNESCO Article 9 therefore supports the disclosure position that AI cannot weaken medical confidentiality by converting confidential information into secondary technical artefacts.
XII.11 UNESCO Universal Declaration on Bioethics and Human Rights, Article 10 — Equality, Justice, and Equity
Source:
UNESCO Universal Declaration on Bioethics and Human Rights, Article 10.
Material source: UNESCO — Universal Declaration on Bioethics and Human Rights.
URL: https://www.unesco.org/en/legal-affairs/universal-declaration-bioethics-and-human-rights
Verbatim / principle:
“The fundamental equality of all human beings in dignity and rights is to be respected so that they are treated justly and equitably.”
Analysis:
The disclosure identifies equality, justice, and equity as engaged where NHS AI systems affect patients differently across disability, age, race, ethnicity, language, accent, digital exclusion, poverty, neurodivergence, sensory impairment, mental-health condition, health literacy, or communication need.
The concern applies to AI triage, app access, voice capture, speech recognition, ambient transcription, AI summaries, automated booking, staff-facing AI systems, and audit interpretation.
The disclosure asserts that average performance is not enough.
AI systems must be safe for the groups most likely to be misheard, excluded, misclassified, delayed, mistranscribed, or unable to challenge outputs.
UNESCO Article 10 therefore supports the disclosure position that NHS AI must be tested for unequal impact before national scaling.
XII.12 UNESCO Universal Declaration on Bioethics and Human Rights, Article 11 — Non-Discrimination and Non-Stigmatization
Source:
UNESCO Universal Declaration on Bioethics and Human Rights, Article 11.
Material source: UNESCO — Universal Declaration on Bioethics and Human Rights.
URL: https://www.unesco.org/en/legal-affairs/universal-declaration-bioethics-and-human-rights
Verbatim / principle:
“No individual or group should be discriminated against or stigmatized on any grounds.”
Analysis:
The disclosure identifies that NHS AI systems may stigmatise patients or workers through classifications, summaries, audit labels, risk flags, access histories, behavioural records, or AI-generated wording.
The concern applies where AI outputs frame a patient as non-compliant, difficult, anxious, aggressive, confused, low priority, digitally disengaged, or unreliable, or where worker AI-use logs are interpreted as incompetence, misuse, delay, or misconduct.
The disclosure asserts that AI-derived language can create institutional stigma even when no human intended it.
Article 11 therefore supports the disclosure concern that AI outputs must be reviewed for dignity, fairness, protected-characteristic impact, and downstream institutional consequences.
XII.13 UNESCO Universal Declaration on Bioethics and Human Rights, Article 15 — Sharing of Benefits
Source:
UNESCO Universal Declaration on Bioethics and Human Rights, Article 15.
Material source: UNESCO — Universal Declaration on Bioethics and Human Rights.
URL: https://www.unesco.org/en/legal-affairs/universal-declaration-bioethics-and-human-rights
Verbatim / principle:
“Benefits resulting from any scientific research and its applications should be shared with society as a whole and within the international community.”
Analysis:
The disclosure identifies benefit-sharing as engaged where NHS patient data, staff data, operational data, clinical pathways, triage records, voice data, correction records, or model-monitoring signals contribute to AI product improvement, commercial value, vendor learning, service optimisation, or public-sector dependency.
The concern is that patients and staff may carry the privacy, safety, and verification risks while external vendors capture operational, commercial, or strategic benefit.
The disclosure asserts that public healthcare data must not become a one-way extraction layer where public risk produces private advantage without transparent public benefit.
UNESCO Article 15 therefore supports the disclosure position that NHS AI deployment must show who benefits, who bears risk, who controls outputs, and how public value is protected.
XII.14 UN Guiding Principles on Business and Human Rights — Corporate Responsibility to Respect Human Rights
Source:
UN Guiding Principles on Business and Human Rights.
Material source: OHCHR — Guiding Principles on Business and Human Rights.
URL: https://www.ohchr.org/sites/default/files/documents/publications/guidingprinciplesbusinesshr_en.pdf
Verbatim / principle:
Business enterprises have a responsibility to respect human rights, avoid infringing on the rights of others, and address adverse human-rights impacts with which they are involved.
Analysis:
The disclosure identifies business-and-human-rights principles as engaged where private vendors, cloud providers, AI model suppliers, SaaS providers, telemetry services, analytics providers, and support providers participate in NHS AI systems.
The concern is that public-sector responsibility does not erase vendor responsibility.
Vendors whose systems process patient data, generate clinical outputs, capture voice, route patients, create summaries, log staff activity, or support NHS workflow must identify and mitigate human-rights risks connected to privacy, equality, safe care, remedy, worker rights, and public accountability.
The disclosure therefore identifies that NHS AI suppliers must show human-rights due diligence, not merely contractual compliance or technical capability.
XII.15 Nuremberg Code — Voluntary Consent and Medical Experimentation Boundary
Source:
Nuremberg Code — ethical principles concerning human experimentation.
Material source: United States Holocaust Memorial Museum — The Nuremberg Code.
URL: https://encyclopedia.ushmm.org/content/en/article/the-nuremberg-code
Verbatim / principle:
“The voluntary consent of the human subject is absolutely essential.”
Analysis:
The disclosure does not assert that ordinary NHS AI deployment is the same as medical experimentation.
The disclosure identifies a boundary issue.
Where AI systems are trialled, piloted, evaluated, optimised, scaled, or improved using patient interactions, clinical data, voice data, staff workflow, triage outcomes, correction records, or model-monitoring signals, the public must be told whether the activity is care delivery, service evaluation, research, product improvement, or experimentation-like deployment.
The ethical concern is that patients and staff must not become involuntary test subjects for AI systems whose safety, accuracy, bias, workload impact, data use, or commercial consequences have not been transparently disclosed.
The Nuremberg principle therefore supports the disclosure position that healthcare AI trials and scaled pilots require clear consent, transparency, governance, and ethical boundary control.
Legal Frameworks Conclusion
This legal-framework conclusion draws together the full framework analysis set out above. It is intended to make the legal architecture readable as a single escalation path, starting with domestic legal foundations and moving outward through common law, statutory rights, healthcare duties, data protection, clinical safety, employment protection, public law, evidential fairness, and international human-rights and bioethical standards.
The purpose of the conclusion is not to repeat every framework in full. Its purpose is to show what the frameworks collectively prove: NHS AI deployment is not ordinary digitisation, routine administration, or a neutral productivity programme. It is a cumulative legal-governance issue because AI systems may process, transform, summarise, infer from, retain, log, monitor, expose, and later evidence confidential medical and staff-related information.
1. Domestic legal foundations
The starting point is domestic lawful-process and confidentiality principle. These frameworks establish that public authority action affecting rights, protected relationships, trust, institutional power, or confidential disclosure must be lawful, evidenced, constrained, and capable of justification.
Key frameworks include:
- Magna Carta principles
- Protected confidentiality principles
- Lawful process
- Evidence over assertion
- Public authority restraint
Applied to this disclosure, these principles mean NHS AI deployment cannot be justified by broad reassurance, policy language, or institutional confidence alone. Where confidential medical data, patient access, staff records, audit trails, or evidence-capable material are processed through AI systems, the lawful basis and evidential foundation must be visible.
2. Common law confidentiality and privacy
The next layer is common law. This is the first operational legal layer because the disclosure concerns information given inside a confidential healthcare relationship.
Key frameworks include:
- Common law duty of confidentiality
- Breach of confidence
- Misuse of private information
Applied to NHS AI, the common law issue is that confidential medical information remains confidential even when it is converted into a prompt, transcript, summary, output, log, telemetry record, support ticket, audit trail, or model-monitoring signal. The legal concern is not limited to whether the original patient record remains protected. It follows the data through the AI processing chain.
3. Human rights
The framework then moves into domestic human-rights law. These rights are engaged because NHS AI systems may affect privacy, records, care access, complaint routes, staff exposure, public-interest speech, and evidential fairness.
Key frameworks include:
- Human Rights Act 1998
- Article 8 — private and family life
- Article 6 — fair hearing
- Article 10 — freedom of expression / public-interest speech
- Article 14 — non-discrimination
- Article 13 — effective remedy
Applied to this disclosure, the human-rights issue is that AI systems may affect a person’s private medical life, ability to challenge records, ability to complain, ability to raise concerns, and ability to obtain remedy. If AI-derived material is hidden, unavailable, uncorrectable, or used without disclosure, the rights become theoretical rather than practical.
4. Equality law
The next layer is equality law. This is required because AI systems may operate unevenly across different patient and staff groups.
Key frameworks include:
- Equality Act 2010
- Disability protection
- Indirect discrimination
- Discrimination arising from disability
- Reasonable adjustments
- Services and public functions
- Public Sector Equality Duty
Applied to NHS AI, equality law requires assessment before deployment and monitoring after deployment. The issue is not whether AI works for an average user. The issue is whether it disadvantages disabled, older, digitally excluded, neurodivergent, accented, language-minority, sensory-impaired, poor, health-literacy-limited, or communication-vulnerable patients and workers.
5. NHS-specific rights and confidentiality governance
The framework then moves into NHS-specific duties. These are central because the disclosure concerns healthcare, not an ordinary commercial service.
Key frameworks include:
- NHS Constitution
- Caldicott Principles
- Patient confidentiality
- Dignity
- Safe care
- Patient involvement
- Purpose justification
- Necessity
- Minimisation
- Strict need-to-know access
- Patient transparency
- Staff responsibility
Applied to NHS AI, these frameworks mean patients must remain informed, protected, involved, and able to trust the system. AI does not reduce NHS confidentiality duties. It increases the number of places where those duties must be proven.
6. Data protection law
The next domestic statutory layer is data protection. This is the core processing framework because NHS AI systems may process personal data, special-category health data, inferred data, generated data, staff data, logs, telemetry, and AI-derived records.
Key frameworks include:
- UK GDPR
- Data Protection Act 2018
- Lawful basis
- Special-category health data
- Transparency
- Access
- Rectification
- Restriction
- Objection
- Automated decision-making
- Data protection by design
- Processor and sub-processor controls
- Security
- DPIAs
- Re-identification risk
- International transfers
- Preservation duties
Applied to NHS AI, the data-protection issue is that compliance must cover the full AI chain, not only the final NHS record or storage location. The relevant question is what data is processed, where it acts, what outputs are generated, who receives or accesses them, how long they are retained, and how patients or staff can access, correct, object, restrict, or challenge.
7. Clinical safety, health IT, medical-device, and records governance
The framework then moves into clinical safety and health-IT governance. This is required because NHS AI may affect care pathways, triage, documentation, patient routing, future treatment, clinical notes, and incident review.
Key frameworks include:
- DCB0129
- DCB0160
- Digital Clinical Safety Assurance
- DTAC
- Medical-device assessment
- MHRA software and AI guidance
- NICE evidence standards
- Duty of candour
- Records management
- Professional duties
Applied to NHS AI, these frameworks mean productivity claims cannot substitute for safety evidence. A tool may save time and still misroute a patient. A tool may reduce queues and still under-triage. A tool may assist documentation and still create inaccurate clinical records. Clinical safety must be evidenced through hazard logs, safety cases, classification assessments, monitoring, correction routes, and traceability.
8. Staff, whistleblowing, and workplace protection
The next layer is staff protection. This is required because NHS AI deployment affects workers as well as patients.
Key frameworks include:
- Employment Rights Act 1996
- Public Interest Disclosure Act 1998
- Health and Safety at Work etc. Act 1974
- Management of Health and Safety at Work Regulations 1999
- HSE stress standards
- ACAS Code
- Mutual trust and confidence
- Employer duty of care
Applied to NHS AI, these frameworks mean staff must not be placed into AI-mediated liability chains without training, role clarity, competence assurance, verification time, workload assessment, audit-use safeguards, disciplinary fairness, stress-risk assessment, reasonable adjustments, and protected-disclosure protection. Staff must not become the accountability endpoint for systems they did not design, procure, configure, govern, or control.
9. Public law, procurement, public money, continuity, and sovereignty
The framework then moves into public governance. This is required because NHS AI deployment is not merely a local IT choice. It may become national public infrastructure.
Key frameworks include:
- Public law rationality
- Proportionality
- Procedural fairness
- Legitimate expectation
- Duty to give reasons
- Algorithmic transparency
- Procurement Act 2023
- Managing Public Money
- Technology Code of Practice
- Sourcing Playbook
- Cloud security principles
- Business continuity
- Sovereign control and exit risk
Applied to NHS AI, these frameworks require public bodies to show rational decision-making, value for money, supplier-risk control, resilience, auditability, portability, transparency, and exit capability. Where AI becomes embedded into patient access, records, triage, staff workflow, audit, and operational planning, dependency becomes a public-law, procurement, and sovereignty issue.
10. Evidential and procedural fairness
The next layer is evidential fairness. This is required because AI systems may generate records that later affect complaints, employment processes, disciplinary action, tribunal proceedings, regulatory reviews, data-rights requests, or legal claims.
Key frameworks include:
- Natural justice
- Right to know and answer the case
- Source-to-output traceability
- Disclosure duties
- Preservation duties
- Authenticity
- Metadata
- Human review
- Automation-bias safeguards
- Litigation prejudice
- Complaint fairness
- Tribunal fairness
- Audit-trail fairness
Applied to NHS AI, these frameworks mean AI-derived material cannot safely be relied upon unless the source chain is preserved and challengeable. Prompts, outputs, transcripts, summaries, logs, telemetry, model versions, audit trails, support records, and human-review notes may all become evidence-capable records. If they are hidden, deleted, overwritten, or treated as system exhaust, procedural fairness is undermined.
11. International human-rights, privacy, bioethics, and business-human-rights standards
The final layer escalates beyond domestic law into international standards. These frameworks do not replace UK law, but they reinforce the public-interest character of the disclosure.
Key frameworks include:
- Universal Declaration of Human Rights
- International Covenant on Civil and Political Rights
- International Covenant on Economic, Social and Cultural Rights
- Convention 108+
- OECD Privacy Guidelines
- UNESCO Bioethics
- UN Guiding Principles on Business and Human Rights
- Nuremberg Code boundary
Applied to NHS AI, these frameworks reinforce privacy, dignity, autonomy, consent, equality, non-discrimination, right to health, worker protection, fair benefit, corporate responsibility, and the ethical boundary between care, research, service evaluation, product improvement, and experimentation. They show that healthcare AI is not only a domestic compliance issue. It is a human-rights, bioethical, and public-trust issue.
Final legal-framework position
The legal frameworks therefore converge on one position:
NHS AI deployment requires proof, not reassurance.
The required proof includes:
- AI system register
- data-flow maps
- lawful-basis assessments
- DPIAs
- equality assessments
- clinical safety cases
- hazard logs
- medical-device classification records
- processor and sub-processor lists
- patient notices
- staff training records
- audit-use protocols
- retention rules
- correction routes
- objection routes
- evidence-preservation rules
- transfer assessments
- procurement justification
- continuity plans
- exit plans
Where those records are absent, undisclosed, incomplete, or untested, the legal-framework concern remains live.
The controlling legal-framework conclusion is:
NHS AI deployment is lawful only where it is transparent, necessary, proportionate, clinically safe, equality-assessed, confidential, accountable, evidence-preserving, staff-protective, patient-rights compliant, procurement-sound, challengeable, and reversible.
Until NHS AI deployment is shown to meet that standard, the disclosure identifies an unresolved public-interest governance risk.
Disclosure Conclusion
This disclosure records a public-interest concern regarding the deployment of artificial intelligence systems across NHS patient access, clinical documentation, triage, staff workflow, administrative processing, audit environments, and healthcare data-processing pathways.
The disclosure does not oppose safe technology.
It opposes the insertion of AI into confidential healthcare systems before the public has been shown the legal, clinical, technical, equality, employment, evidential, procurement, and sovereignty safeguards required to make that deployment lawful, safe, transparent, accountable, challengeable, and reversible.
1. The central issue
The central issue is not ordinary NHS digitisation.
The central issue is that AI systems may now sit between:
- the patient and the clinician;
- the patient and access to care;
- the clinician and the clinical record;
- the worker and the audit trail;
- the NHS and external vendors;
- the public healthcare system and foreign-controlled infrastructure;
- the original source material and later evidential reliance.
That changes the nature of NHS data governance.
AI systems do not merely store data.
They act on data.
They process, infer, summarise, classify, route, log, monitor, retain, expose, and produce outputs from patient symptoms, consultation speech, clinical records, staff prompts, access histories, workflow material, audit trails, and operational signals.
2. Patient-side consequence
For patients, the disclosure identifies a risk that confidential medical information may be processed through AI systems before patients have been clearly told:
- what AI system is being used;
- what data it processes;
- whether voice is captured;
- whether AI affects triage or routing;
- whether AI-generated summaries enter the record;
- whether logs, telemetry, or support records are created;
- who can access the data;
- how long records are retained;
- how errors can be corrected;
- how AI processing can be objected to;
- whether an equivalent non-AI route exists.
A patient may believe they are speaking to a clinician, submitting symptoms to the NHS, or using an ordinary access route.
But if AI systems process that information through vendor-supported, cloud-based, model-mediated, telemetry-producing, or audit-generating pathways, then the patient is not only interacting with the NHS.
They are entering an AI processing chain.
That chain must be disclosed.
3. Staff-side consequence
For staff, the disclosure identifies a risk that NHS workers may be placed into AI-mediated liability structures without adequate training, role clarity, workload assessment, audit-use safeguards, protected-disclosure protection, or disciplinary fairness.
Staff may be expected to:
- use AI tools;
- input prompts;
- verify AI outputs;
- correct AI-generated summaries;
- approve records;
- manage patient confidentiality;
- interpret audit logs;
- defend AI-derived records;
- carry responsibility for errors originating upstream.
That creates a liability displacement risk.
Staff must not become the accountability endpoint for AI systems they did not design, procure, configure, govern, or control.
4. Clinical safety consequence
For clinical safety, the disclosure identifies that AI systems affecting triage, routing, clinical documentation, ambient voice capture, summarisation, record formation, or future care must be supported by visible safety evidence.
Productivity claims are not clinical safety evidence.
Queue-reduction claims are not clinical safety evidence.
Pilot success is not national safety evidence unless the clinical hazards, equality risks, under-triage risks, mistranscription risks, hallucination risks, escalation thresholds, incident records, correction routes, and post-deployment monitoring are visible.
Where AI affects care, the NHS must show the safety case.
5. Equality consequence
For equality, the disclosure identifies that NHS AI systems may affect patients and workers differently depending on disability, age, race, ethnicity, language, accent, sensory impairment, neurodivergence, mental-health condition, poverty, digital exclusion, health literacy, and communication need.
AI cannot be declared safe because it works for average users.
The relevant question is whether it works safely for the people most likely to be excluded, misheard, mistranscribed, misclassified, delayed, routed incorrectly, unable to challenge outputs, or unable to access digital-first routes.
If those assessments are absent, the equality risk remains live.
6. Data protection and confidentiality consequence
For data protection and confidentiality, the disclosure identifies that confidential medical information remains protected even when converted into AI-derived material.
That includes:
- prompts;
- outputs;
- transcripts;
- summaries;
- logs;
- telemetry;
- support tickets;
- audit trails;
- model-monitoring records;
- correction histories;
- routing decisions;
- generated clinical notes.
The disclosure therefore adopts the following principle:
The breach is not where the data rests. The breach is where the data acts.
A storage-location assurance is incomplete if the data acts elsewhere through AI execution, inference, logging, telemetry, support access, model monitoring, or later evidential reliance.
7. Re-identification consequence
The disclosure further identifies that pseudonymisation, anonymisation, masking, or name removal does not automatically remove AI-era identity risk.
AI systems can infer identity through pattern.
Relevant patterns may include:
- symptom sequence;
- rare condition;
- medication;
- appointment timing;
- postcode area;
- age;
- voice;
- accent;
- disability-related communication;
- clinical pathway;
- staff behaviour;
- audit logs;
- prompts;
- telemetry;
- system usage.
The disclosure therefore adopts the following principle:
In AI systems, the pattern is the person.
8. Evidential consequence
The disclosure identifies that AI-derived records may become evidence-capable.
They may affect:
- patient complaints;
- clinical safety reviews;
- subject access requests;
- rectification requests;
- disciplinary processes;
- capability assessments;
- protected disclosures;
- employment disputes;
- tribunal proceedings;
- regulatory investigations;
- legal claims.
If AI-derived material is relied upon, the source chain must be preserved and disclosed.
The required chain is:
source material → input / prompt → AI system → output → human review → edit history → final record → audit trail → later reliance.
Without that chain, AI evidence is procedurally unsafe.
9. Procurement and sovereignty consequence
For procurement and sovereignty, the disclosure identifies that NHS AI deployment may create dependency on external vendors, SaaS providers, cloud infrastructure, AI model providers, telemetry systems, support providers, analytics providers, and foreign-controlled infrastructure.
That dependency is not merely commercial.
It may affect patient access, staff workflow, clinical records, triage, documentation, audit, operational planning, and continuity of public healthcare.
Where AI systems become embedded into NHS infrastructure, the public must be shown:
- the procurement justification;
- the value-for-money assessment;
- the vendor chain;
- the processor and sub-processor chain;
- the cloud and support-access model;
- the data-portability terms;
- the exit route;
- the continuity plan;
- the sovereign-control safeguards.
If the NHS cannot exit safely, the system is not merely a tool.
It is a dependency.
10. Required public proof
This disclosure therefore requires proof, not reassurance.
The required proof includes:
- AI system register;
- data-flow maps;
- lawful-basis assessments;
- DPIAs;
- equality assessments;
- clinical safety cases;
- hazard logs;
- DTAC assessments;
- medical-device classification records;
- processor and sub-processor lists;
- patient notices;
- staff training records;
- audit-use protocols;
- retention rules;
- correction routes;
- objection routes;
- human-review routes;
- evidence-preservation rules;
- incident records;
- transfer assessments;
- procurement justification;
- continuity plans;
- exit plans.
Without those records, public assurance remains assertion.
11. Final disclosure position
This disclosure is made in the public interest because NHS AI deployment affects confidential medical data, patient rights, clinical safety, equality of access, staff protection, whistleblowing, evidential fairness, public spending, procurement accountability, critical infrastructure resilience, and sovereign control over healthcare processing.
The central accountability question is:
Has AI been deployed into NHS healthcare before the public has been shown how it is lawful, safe, fair, transparent, accountable, challengeable, and reversible?
Until that question is answered with records, the public-interest concern remains unresolved.
The disclosure conclusion is therefore straightforward:
NHS AI deployment must not proceed as hidden infrastructure inside healthcare access, clinical records, staff workflow, audit trails, or public administration unless the full legal, clinical, technical, equality, employment, evidential, procurement, and sovereignty safeguards are visible, tested, and enforceable.
Structural Impact Formula
The Structural Impact Score ($SIS$) is defined as:
$SIS = \left( w_T + w_V + w_R + w_I \right)\left( 1 + \lambda \cdot 6 \right)$
Where:
- $T$ = Tribunal / Welfare Disruption
- $V$ = Vulnerability Amplifier
- $R$ = Rights / Regulatory Misstatement
- $I$ = Institutional Interlock
The interaction multiplier $\left(1 + \lambda \cdot 6\right)$ reflects $\binom{4}{2} = 6$ co-occurring structural interaction pairs.
Structural Impact Result
Activated Structural Variables:
$T = 1,\; V = 1,\; R = 1,\; I = 1$
Interaction Pair Count: $\binom{4}{2} = 6$ distinct co-occurring structural interaction pairs.
Resolved Structural Impact Score:
$SIS = \left( w_T + w_V + w_R + w_I \right)\left( 1 + \lambda \cdot 6 \right)$
The disclosure records concurrent activation across tribunal and welfare disruption, medical and disability vulnerability, rights and regulatory governance, and institutional interlock throughout the NHS AI ecosystem. The structural conditions arise from the interaction between healthcare delivery, patient-data processing, AI-assisted clinical systems, public-sector governance, technology vendors, cloud infrastructure, and the downstream legal, employment, welfare and tribunal consequences associated with AI-generated medical information and healthcare decision-making.
Structural Impact Meaning
An $SIS$ produced by four concurrently active structural variables with $\binom{4}{2} = 6$ interaction pairs indicates a compound public-service governance condition rather than an isolated healthcare technology or data-processing issue.
The co-activation of tribunal and welfare disruption $T$, vulnerability amplification $V$, rights and regulatory misstatement $R$, and institutional interlock $I$ demonstrates mutually reinforcing structural failures across healthcare delivery, patient-data governance, disability protection, AI-assisted clinical systems, employment and tribunal consequence, public-sector accountability, and medical data sovereignty.
The interaction multiplier $\left(1 + \lambda \cdot 6\right)$ confirms non-linear escalation. Healthcare and welfare obligations increase the significance of medical vulnerability; regulatory and legal duties amplify failures in AI governance and patient-data processing; and institutional interlock extends those effects across NHS organisations, technology vendors, cloud infrastructure, regulators and connected public bodies.
This represents a cumulative systemic condition in which healthcare, welfare, disability protection, legal governance and interconnected institutional decision-making operate together to increase the risk of unlawful processing, unsafe AI-assisted clinical outcomes, procedural disadvantage, evidential prejudice, reduced public accountability and continuing erosion of medical data sovereignty.